
Comparison of Ibuprofen and Celecoxib For Controlling Post Endodontic Pain
INTRODUCTION
The relationship between pain and dentistry is frequently portrayed in popular culture as synonymous with situations to be avoided. In fact, poorly controlled dental pain and related anxiety contribute to postponed or cancelled appointments[1],[2]. Dental fear is a major reason given for avoiding dental visits[3]. Effective control of dental pain improves patient comfort, facilitates the delivery of oral care, decreases anxiety, and may even improve oral health. The aim of root canal treatment is to eliminate bacteria from the canal system in order to create an environment favorable for healing. Current preparation techniques along with disinfectants or medicaments may disrupt the intra-canal microbial environment. However, numerous studies have shown that it is impossible to achieve a bacteria free root canal consistently1-[4]. Hence, there is concern over the consequences of the presence of the remaining microorganisms in the canal.
It is generally believed that the remaining bacteria can be either eradicated or prevented from recolonizing the root canal system through an inter-appointment medicament such as calcium hydroxide2,5. However, it has been demonstrated that calcium hydroxide consistently fails to sterilize root canals and may even allow regrowth in some cases3,4,6. The presence of cultivable microorganisms at the time of obturation has been reported to impair healing after root canal therapy 7. Certain factors such as preoperative pain2 use of intra-canal medications5,6 and tooth localization may predispose the development of inter and post appointment pain. Mechanical instrumentation is the core method for bacterial reduction in the infected root canal. Various treatment regimens for the relief of pain during endodontic therapy, includes pre-medication relief of occlusion, establishment of drainage, intra-canal and systemic medications. Preparation of root canal systems includes both enlargement and shaping of the complex endodontic space together with its disinfection. A variety of instruments and techniques have been developed and described for this critical stage of root canal treatment. The advantages of conventional hand instrumentation from crown to apex with early coronal flaring include less risk of inoculation of endodontic pathogens in the periradicular tissues, enhanced penetration of irrigant into the root canal system, less extrusion of irrigant solution and furthermore there is less likelihood for a change in the working length measurement during preparation, greater tactile awareness and reduced coronal binding of instruments. On the other hand the step-back technique creates a smoother flow and a tapered preparation from apical to coronal direction. Our study is comparing the inter-appointment pain in vital single rooted teeth by using two classical techniques used for root canal preparation. These techniques are crowndown or step-down and apical step-back. The frequency of pain will be assessed by employing visual analogue pain scale to compare the two groups8. Knowledge on the causes and the mechanisms behind inter-appointment pain is very important for the practitioner to manage this undesirable condition. Inter-appointment emergency, proper diagnosis and active treatment is required for the clinician to overcome the problem. It is therefore important to carry out a study, which can help us in improving our knowledge and skills regarding the precise diagnosis as well as the management of inter-appointment pain. Previous local studies are limited in this regard.
METHODOLOGY
Patients were selected from out-door patients coming to operative dentistry department of Liaquat University of Medical and Health Sciences, Jamshoro.
After taking the inclusion and exclusion criteria into consideration, detailed history were taken and all necessary investigations were done. Pre-operatively, the tooth could not always be accurately diagnosed as vital or non vital by history taking, clinical and radiographic examination and vitality testing, therefore the gold standards of diagnosis was a presence of bleeding from the pulp chamber and the root canals determined by direct observation after access opening, Cases with non vital pulp were selected in this study.
Two standardized peri-apical radiographs were taken during the treatment, as follows:
- Pre-treatment.
- Working length determination with files in situ. Local Anesthesia has been administered and rubber dam applied for isolation. Adequate coronal access into the pulp chamber was made in order to provide easy access of endodontic instruments to all the walls of the root canals.
This was achieved by using high speed hand piece with a number 2 round bur and tapered fissure bur (Alpha Dental Diamond burs USA Certified ISO 9002) for both crown down and step back technique groups. To achieve the working length we used a distance of 1 to 2mm short of the apex to limit our canal preparations and obturation. According to the size of the image of the tooth on the preoperative radiograph, a file was inserted into each root canal so that it would reach approximately within 2mm of the radiographic apex.
From instrument tip to stopper, this length was measured when in the canal the stopper was rested against a reference point. A working length radiograph was subsequently obtained. Correct working length was obtained by observing the distance between tip of the file and radiographic apex.
Canals have been instrumented using a crown-down in the first group by first flaring the coronal third of each tooth with gates gladden bur No (2-4) (Dentsply, Millefer, Switzerland) while middle and apical third was prepared by hand files (Kerr, Romulus, Mich.) along with irrigant using 5.2% sodium hypochlorite solution and step-back technique in the second group by conventional handfiles on apical and middle third and then the coronal third of each tooth were flared with gates gladden bur No (24) (Dentsply, Millefer, Switzerland) along with irrigant using 5.2% sodium hypochlorite solution. The canals dried and the teeth were temporized by temporary filling material cavit (provis, Favodent karl Huber GmbH, Germany) and patient were recalled for next appointment to complete the root canal procedure, in case of severe pain, symptomatic treatment were given.
The patients were assigned into group A or B by envelope method. Group A had their root canals prepared by crown down and group B by step-back. The patients were telephonically accessed to record the pain after 24 hours and 48 hours after the initial treatment. The data were collected on the Performa.
Data were collected and entered in SPSS version 10 for windows. Mean ± SD were presented for age of the patient and VAS. Male to Female ratio were presented for gender distribution. Chi-squared test were used to compare VAS between the two groups. A p-value of <0.05 was considered as statistically significant.
RESULTS
A total of 60 patients required endodontic treatment with vital teeth were included in this study and canals were instrumented using a crown-down and step-back technique. Subjects were equally divided into two groups by using envelope method, for group A, root canals prepared by crown down and group B by step-back. The average age of the patients was 32.83 ± 9.23 years (30.45 to 35.22). The average age of the patients was significantly high in group A than group B (40.50 ± 5.51 vs. 25.17 ± 4.64 p=0.0001). Out of 60 patients, 22(36.7%) were male and 38(63.3%) were female. Proportion of gender was not significant between groups (p=1.00). Regarding maxillary and mandibular tooth location thirty three (55%) maxillary teeth were treated and 27(45%) mandibular teeth were treated.
Comparison of inter appointment pain at 24 hrs and 48 hrs between groups are presented in table 1 . Inter appointment pain at 24 hrs was found in 35% (21/60) patients. In group A (crown down technique), inter appointment pain was only in 23.3% (7/30) patients and in group B (step back technique) in 46.7% (14/30) patients. Rate of inter appointment pain was high in group B than group A but it is not statistically significant (chi-square =3.59; p=0.058). In the other word inter appointment pain was 2.87 times more likely in step back technique (group B) than crown down technique (OR=2.87; 95%CI: 0.95 to 8.69).
At 48 hours, inter appointment pain was observed in 40% (24/60) patients. In group A inter appointment pain was in 40% (12/30) patients and in group B in 40% (12/30) patients. Rate of inter appointment pain was not
TABLE 1
COMPARISON OF INTER APPOINTMENT PAIN BETWEEN GROUPS

statistically significant between the group at 48 hours (chi-square =0.0001; p=1.00). In the other word odd ratio is 1 (OR=1.00) its mean pain was equally likely in both groups (OR=1; 95%CI: 0.35 to 2.81).
Comparisons of inter appointment pain at 24 hrs and 48 hrs between groups after stratification of gender, age groups and location were presented in table 2 and 3. Gender and age groups were not effect on pain between groups. In Maxillary teeth, pain was significantly high
TABLE 2
COMPARISON OF INTER APPOINTMENT PAIN BETWEEN GROUPS AT 24 HOURS AFTER CONTROLLING GENDER, AGE AND LOCATION OF TEETH
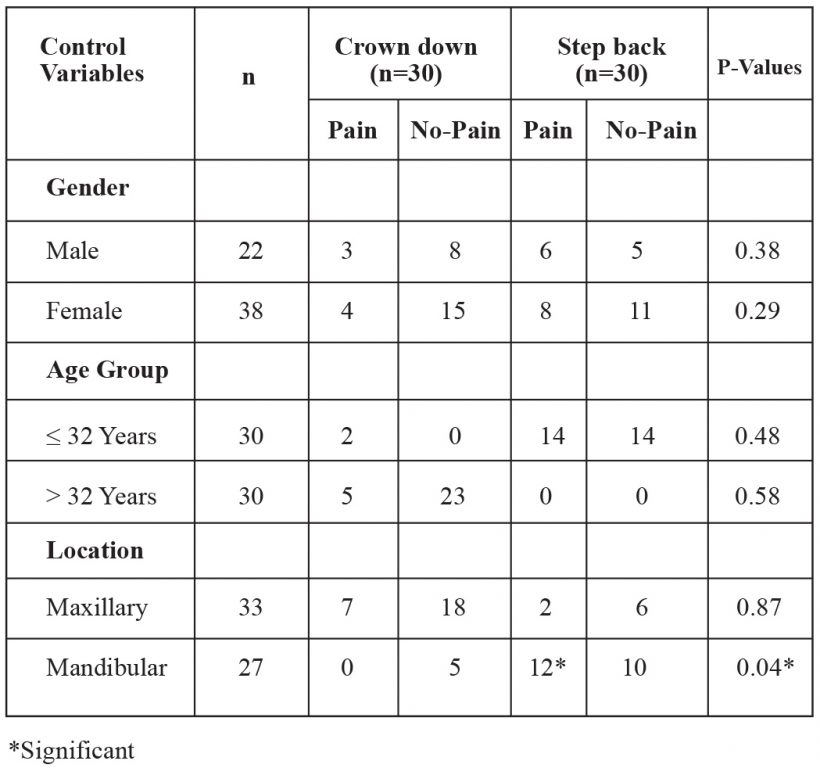
TABLE 3
COMPARISON OF INTER APPOINTMENT PAIN BETWEEN GROUPS AT 48 HOURS AFTER CONTROLLING GENDER, AGE AND LOCATION OF TEETH

in step back technique than crown back technique (fisher’s exact test; p=0.04) at 24hours. In mandibular teeth, pain was significant at 24hour while at 48hours it was not significant.
DISCUSSION
Inter appointment pain was and remains one of the most common problems in endodontic treatment procedure although these in most cases do not last long, but could be a source of embarrassment to the dentist and annoying for the patient. Some studies investigating inter appointment pain have reported an incidence of moderate to severe pain in the range of 15% to 25% 7-9. Studies also have reported frequencies of inter appointment emergencies ranging from 1.4% to 16% 1. While in our study discomfort to mild inter appointment pain noted from 35%to 46.7%. In this study the frequency of inter appointment pain has been assessed by visual analogue pain scale to compare crown-down and stepback techniques10. Knowledge on the etiological factors and the mechanisms behind inter appointment pain is very importance for the practitioner to properly prevent or manage this undesirable condition. One of this etiological factor is the preparation techniques and their effect on the amount of the debris being extruded through the apical foramina which plays very important role in the frequency of inter and post operative pain. In this study we have found that after the preparation with crown-down and step-back techniques, the rate of inter appointment pain was high in group B (step-back) than group A (crown-down) but it is not statistically significant. Although the rate of the inter appointment pain was high after using step-back technique and that could be due to the amount of the debris pushed beyond the apex or the technique was not able to produce 100% environment free of microorganism it was not enough to bring the result to the significant level. In comparative study between both technique by the quantitative assessment of canal debris forced periapically instrumentation Ruiz-Hubard EE,et al11 concluded that step-back technique reported to produce more debris
apically than crowndown. Ferraz CC, et al12 also have found in their study that apical extrusion of debris and irrigants using two hand and three engine-driven instrumentation techniques were more in step-back as it compare with crown-down technique.
Reddy S, Hicks L13 also they have concluded in their study that crown-down extruded less debris after comparing the debris extruded from the apical constriction using two hand and two rotary instrumentation techniques.
It is well understood that the pain has direct relation with status of the pulp pre operatively and the sign/symptoms. In our study the criteria we have taken were included only Non vital cases and we have found that the inter appointment pain was presented in 35% of the cases within the first 24 hrs and 40 % within 48 hrs but in both it was not significant and the intensity of the pain was noticed to vary from degree of discomfort to mild pain and that does not require any analgesic, it was also observed that the pain disappeared slowly and gradually by the end of the root canal procedure.Walton& Fouad et al14 have found that the frequency of flare-ups or interappointment pain in necrotic pulp cases were significantly high as compare with to vital cases. Naidoff also has discuss briefly how necrotic pulp plays role in the development of antibodies-antigens reaction which lead to cascade of complement system and inflammatory reaction resulting in flare-up or inter appointment pain15. So many studies have founded that the incidence of flare-up is more with non vital pulp as it compare with vital.
As the age of the patients is concern in this study we have found that there is no relation between the age of the patients and the inter appointment pain which means that there was no statistically significant differences observed in different age groups in this study. Eleazer PD, Eleazer KR and Matusow also concluded that there is no significant relationships for inter appointment flareups with age3. Several studies also have failed to find any relation between ages and inter appointment pain Walton R, and Fouad A14. In their study have found no relation between flare-up and age of the patients Imura N and Zolo M16 have also concluded the same result. Toosy17 who treated necrotic teeth and found no difference in flare-ups rate of age groups except in those patients who were above 50 year. Kane 18 has found no relationship between
post obturation pain and age. The reason could be due to a coronal transportation of the radiographic apex because of secondary cementum deposition with advancing age. This would result in an error of working length determination which could lead to extrusion of debris and inter or post preparation pain. After all in the current study and the above discussed studies we have concluded that there is no scientific evidence indicating that age is risk factor in the development of inter appointment pain.
As far as the relation of the pain to gender is concerned, In this study, we have found no relation between the gender and inter appointment pain which meant that there is no significant relation between gender and inter appointment pain and the reason may be due to the small sample size of patients being assessed in our study. However several studies have shown significant relationship where larger sample size of patients were examined 4,19,20.
Morse et al21, Mulhern et al22, Albashaireh and Alnegrish 2 had similar results that we have found in our study but Fox et al23 and Genet et al20 concluded that the incidence of flare-up in females are more as compare to males.
Although it’s hard to believe that women suffer from psychomatic illness but physicians believe that their pain is directed by their emotional status24. Also the biological differences between genders explain the high incidence of pain in female as it compare to male25. The reasons maybe due to difference in pelvic and reproductive organs which may provide an additional portal of entry of infection in females leading to possible local and distant hyperalgesia26. And the fluctuation in female hormonal levels, which may be associated with changing in the levels of serotonin and nor-adrenaline, causing increase in pain during the menstrual period27,28. Our study has concluded that gender difference and females’ predominance in the frequency of inter appointment pain is more but it is not statistically significant. In this study the frequency of inter appointment pain is more in the mandibular as it compare to maxillary teeth. In mandibular teeth pain was significant at 24 hour while at 48 hours it was not significant.
Kane18 found no correlation of post obturation pain with tooth type and that totally opposite to the result that we have concluded which similar to the result of Walton14, Toosy17, Fox23, Mollar29 and Barnett30 There is possible explanations for more pain in mandibular teeth as it compare to the maxillary teeth and that is the cortical thicker plate of the mandible which may cause accumulation of exudates, causes more pressure as compared to maxilla.
CONCLUSION
The result of this study shows no significant difference in inter-appointment pain between crown-down preparation technique and step-back technique.
LEGENDS
Table I: comparison of inter appointment pain at 24 & 48 hrs between groups.
Table II: comparison of inter appointment pain between groups at 24 hours after controlling gender, age and location of teeth.
Table III: comparison of inter appointment pain between groups at 48 hours after controlling gender, age and location of teeth.
REFERENCES
- Siqueira JF Jr, Rocas IN, Favieri A, Machado AG, Gahyva SM, Oliveira JC, Abad EC. Incidence of post operative pain after intracanal procedures based on an antimicrobial Strategy. J Endod 2002; 28:457-460.
- Albashaireh ZS, Alnegrish AS. Post obturation pain after single- and multiple-visit endodontic therapy. A prospective study. J Dent 1998; 26:227-232.
- Eleazer PD, Eleazer KR. Flare-up rate in pulpally necrotic molars in one-visit versus two-visit endodontic treatment. J Endod 1998; 24:614-616.
- Trope M. Relation of intra-canal medicaments to endodontic flare-ups. Endod dent tarumatol 1990;6:226-229
- Abott PV. Medicaments: aids to success in endodontics part 1. A review of literature. Aust Dent J 1990;35:438-448.
- Tayfun A, Ali CT . Interappointment Emergencies in teeth with necrotic pulps. J Endod 2002; 28:375-377. 7. Clem W: Post-treatment endodontic pain, J Am Dent Assoc, 1970; 81:1166–1670.
- Harrison J, Baumgartner J, and Svec T: Incidence of pain associated with clinical factors during and after root canal therapy. 1. Interappointment pain, J Endod 1983;9:384387.
- O’Keef E: Pain in endodontic therapy: preliminary study, J Endod 1976;2: 315-319.
- Chapman HR, Kirby-Turner N. Visual/verbal analogue scales: Examples of brief assessment methods to aid management of child and adult patients in clinical practice. Br Dent J 2002; 193: 447-450.
- Breivik EK, Barkvoll P, Skovlund E. Combining diclofenac with acetaminophen or acetaminophen-codeine after oral surgery: a randomized, double-blind singledose study. Clin Pharmacol Ther 1999; 66: 625-635.
- Hargreaves KM, Keiser K. Development of new pain management strategies. J Dent Educ 2002: 66: 113- 121. 13. Reddy S, Hicks L. Apical extrusion of debris using two hand and two rotary instrumentation techniques. J Endod 1998;24:180-183.
- Walton R, Fouad A. Endodontic interappointment flare-ups: a prospective study of incidence and related factors. J Endod 1992;18:172-177.
- Naidorf IJ. Endodontic flare ups : Bacteriological and immunological mechanisms. J Endod, 1985;11: 462 – 464.
- Imura N, Zuolo M. Factors associated with endodontic flare-ups: a prospective study. Int Endod J 1995;28:261-265.
- Toosy A. Flare-up rate in pulply necrotic molar in one visit versus two visit endodontic treatment. Dessertation;2002.
- Kane AW, Sarr M, Faye B, Toure B, Ba A. incidence of post operative pain in single session root canal therapy (study in black Senegalese apropos of 96 cases). Dakar Med 1999; 44:114-118.
- Torabinejad M, Kettering JD, McGraw JC, Cummings RR, Dwyer TG, Tobias TS. Factors associated with endodontic interappointment emergencies of teeth with necrotic pulps. J Endod 1988: 14: 261-266.
- Genet JM, Hart AA, Wesselink PR, Thoden van Velzen SK. Preoperative and operative factors associated with pain after the first endodontic visit. Int Endod J 1987;20:53-64.
- Morse DR, Furst ML, Belott RM, Lefkowitz RD, Spritzer IB, Sideman BH. Infectious flare-ups and serious sequelae following endodontic treatment: a prospective randomized trial on efficacy of antibiotic prophylaxis in cases of asymptomatic pulpal-periapical lesions. Oral Surg Oral Med Oral Pathol 1987; 64:96-109.
- Mulhern JM, Patterson SS, Newton CW, Ringel AM. Incidence of postoperative pain after one-appointment endodontic treatment of asymptomatic pulpal necrosis in single rooted-teeth. J Endod 1982;8:370-375. 23. Fox J et al. Incidence of pain following one visit endodontic treatment. Oral Surg 1970;30:123-125. 24. Colemeco S, Becker LA, Simpson M. sex bias in the assessment of patient’s complaints. J Fam Pract 1983; 16:1117-1121.
- Fillingim RB, Maixner W. Gender difference in the responses to noxious stimuli. Pain Forum 1995; 4:209221.
- Berkley KJ. Sex differences in pain. Behaviour and Brain Science 1997; 20:371-380.
- Marcus DA. Interrelationships of neuro-chemicals, estrogen, and recurring headache. Pain 1995; 26:129139.
- Dao TTT, Knight K, Ton-That V. Modulation of myofascial pain patterns by oral contraceptives: a preliminary reports. J Dent Res 1997; 76:148.
- Mollar A, Fabricus L, Dahin G, Ohman A, Heyden G. Influence on periapical tissues of indigious oral bacteria and necrotic pulp tissues in monkeys. Scand J Dent Res 1981; 89:475-484.
- Barnett F, Tronstad L. The incidence of flare-ups following endodontic treatment. J Dent Res 1989; 68:1253.