
Relation of Vibrating Line to Location of Fovea Palatinae in Local Population
INTRODUCTION:
Although a lot of patients maintain good care of their teeth but still many patients require dental prostheses in the oral cavity to establish esthetics, speech, mastication and to restore the lost structure of the oral cavity like teeth, mucosa and ridge.1 The oral cavity of every
individual is unique with respect to anatomical landmarks, yet there are more innovations with respect to area and genetic differences in populations of that specific area. Therefore, proper evaluation of landmarks provides positive guidance in the fabrication of denture and population-related differences for the specifically constructed prosthesis. The removable denture is expected to satisfy fundamental principles of retention, support, stress distribution and also of tissue preservation. Successful prosthodontic treatment requires dental prosthesis to be retentive.2
Retention of the denture is defined as “resistance of a denture to vertical movement away from the basal tissues’ and as ‘that quality inherent in the prosthesis acting to resist the forces of dislodgement along the path of insertion.2 ” Contributory factors in removable denture retention are atmospheric pressure, surface tension, vacuum, adhesion, cohesion, viscosity, border seal, base adaptation, seating
force and muscular control. Among these most important factors for retention are good base adaptation and border seal.2,3 In upper complete denture, good base adaptation and the posterior palatal seal of the denture are formed to bring denture into contact with adjacent oral tissues to exclude the air from between the denture and the supporting mucosa. This will establish an effective valve seal.4
Fovea palatinae are the mucous gland in the maxilla. This anatomical landmark can be located as two small pits (fovea palatinae) one on either side of the midline on the anterior part of the soft palate in maxilla.4,5 Mostly during the procedure of insertion of a denture, fovea palatinae is given relief for removal of pressure on this specific area. The posterior limit of maxillary complete denture has a great impact with respect to the location of fovea palatinae.5,6 The fovea palatine should not be covered in patients with thick and ropy saliva since the thick consistency of saliva makes denture unretentive due to increased hydrostatic pressure. Fovea palatinae are located in close proximity to the vibrating line and considered as useful guide.7 The Vibrating line is an imaginary line located on the posterior part of the palate, differentiating between moveable and immovable tissue of the soft palate.3,4,5,6,7,8 It extends from one hamular notch to the other. The vibrating line can be identified when the soft tissue in the palate is moving and are used to clinically establish the posterior extent of the maxillary complete dentures.9 The location of the vibrating line can be detected by using different techniques.
. Phonation ‘Ah’ sound
. Nose blowing method
. Swallowing method10
A vibrating line can be located by asking the patient to say AH with short intervals not vigorously but in small bursts. It is a curved line between both hamular processes. Mostly it is carved in a butterfly shape. The vibrating line makes the most posterior extension of maxillary denture base.11
According to Boucher, fovea palatinae are always present in soft tissue and close to the vibrating line that is the best guide for the posterior denture extension.12 The prosthodontists had consensuses about the relation between the posterior border of the maxillary denture and vibrating line.13 The posterior palatal seal is located in the soft tissue at thebjunction of the hard and soft palate on which the posterior
part of the maxillary denture can insert pressure within the physiological limit of tolerance on tissue, which will ultimately help to improve the retention of the denture GPT).14 It provides stability, retention, compressibility and comfort.
The posterior palatal seal is three-dimensional area where pressure within tolerable limits of the tissues can be applied, to increase retention of the maxillary removable denture by providing an effective seal, prevents food entrapment under the denture base, reduces gagging, makes the palatal border of maxillary denture less problematic to the tongue.11,15,16
The anteroposterior dimension of the posterior palatal seal is influenced by the type of soft palate which indicates the broad, medium and narrow posterior palatal seal area respectively. The soft palate is classified as
1. Class 1: it indicates horizontal soft palate with a
10-degree angle to the hard palate that is with very less
muscular activity
2. Class 2: palatal contour lie between class 1 and class
3 and have around a 45-degree angle to the hard palate
3. Class 3: it indicates a high v-shaped palatal vault with around a 75-degree angle to the hard palate.17
There are several ways for the establishment of the seal at the posterior palate. The technique that is mostly used is by marking the vibrating line when the patient says ah.3,6,9,17,18 In this approach, the dentist draws a line with an indelible pencil through pterygomaxillary notch anterolaterally when the patient pronounces ah sound in short bursts, then the moveable and immovable part of the palate is visible.3,6,9,18
METHODOLOGY:
Inclusive criteria
The patients which were included are
. Both gender [male and female]
. The age range of 20 to 79 years
. The normal pink color palatal mucosa with clinically visible fovea palatinae
Exclusive criteria:
The patients which were excluded from the study are
. Patients with a history of surgery/ trauma in the craniofacial region.
. Patients with acquired and congenital craniofacial defects
. The patient presented with any pathology or inflammation of palatal mucosa
. The patient presented with limited mouth opening
This cross-sectional observational study sample size was two hundred and fifty patients dentate, partially dentate and edentate. The sample size was calculated according to sample size determination in health studies; a practical manual of World Health Organization (WHO) Genava5. There are many methods to evaluate fovea palatine, vibrating line, and posterior palatal seal but in this study, the most convenient
method with the marking of the ‘Ah’ line in patients is used. People who could pronounce the “Ah” sound repeatedly with their mouths open were considered in this study. After individual’s education and counseling, written Informed consent was obtained from them before including them in the study. All patients were examined and the individual patient was seated on a dental chair, turned on dental unit
light for proper illumination inside the oral cavity. The individual was instructed to be seated in a normal relaxed position and wide open his/her mouth. With the help of gauze, the palatal mucosa was dried before any evaluation. Initially, it was determined whether the foveae palatinae was visible or not visible in the soft palate mucosa and then the position of foveae palatinae was marked. The researcher marks the palate with an indelible pencil to record the vibrating line across the soft palate by asking the patient to say “Ah” repeatedly with the mouth open. In the end, the relationship of the vibrating line with the fovea palatinae was identified and the distance of fovea palatinae was
measured with a divider. The findings were recorded in proforma as to whether fovea is present anterior, posterior or at the vibrating line and the distance with vibrating line was also measured. The procedure was repeated twice to verify the accuracy of markings.
RESULTS:
The results were analyzed using SPSS Version 23. The mean age of the male and female patients was calculated. Mean distance of fovea palatinae to ah line in both the gender were calculated. Then the frequency of various location of fovea palatinae with respect to vibrating line were calculated. The fovea palatinae mostly existed 1.68 mm1.11 anterior to the vibrating line. The mean age of the male patients in
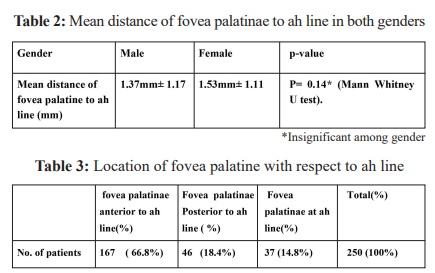
this study was 34.41years 15.82, while that of female patients was 30.15 years 11.99. There was no statistically significant difference between the mean ages of both genders.P=0.072 (Mann Whitney U test) Table 1. The mean distance of the fovea palatine to ah line in male patients was
 1.37mm± 1.17 while in females was 1.53mm 1.11. We found no statistically significant difference between the mean distance in both genders. P= 0.141 (Mann Whitney U test) Table 2. Out of total number of 250 patients (n= 250), 167 patients (n=167) 66.8% have fovea palatinae anterior to vibrating line (ah line), 46 patients (n= 46) 18.4% have fovea palatinae posterior to vibrating line (ah line) and 37 patients (n=37) 14.8% have fovea palatinae at vibrating line (ah line).
1.37mm± 1.17 while in females was 1.53mm 1.11. We found no statistically significant difference between the mean distance in both genders. P= 0.141 (Mann Whitney U test) Table 2. Out of total number of 250 patients (n= 250), 167 patients (n=167) 66.8% have fovea palatinae anterior to vibrating line (ah line), 46 patients (n= 46) 18.4% have fovea palatinae posterior to vibrating line (ah line) and 37 patients (n=37) 14.8% have fovea palatinae at vibrating line (ah line).

 Â Â In Figure 1, the Mean distance of fovea palatinae to ah line when fovea is anterior to ah line is 1.68mm 1.11, Mean distance of fovea palatinae when it is posterior to ah line is 1.52mm 0.95.T test was used to compare the mean distances p= 0.38. The result is not significant that is there is no statistically significant difference between the mean distance of fovea palatinae to ah line (vibrating line) regardless of its
  In Figure 1, the Mean distance of fovea palatinae to ah line when fovea is anterior to ah line is 1.68mm 1.11, Mean distance of fovea palatinae when it is posterior to ah line is 1.52mm 0.95.T test was used to compare the mean distances p= 0.38. The result is not significant that is there is no statistically significant difference between the mean distance of fovea palatinae to ah line (vibrating line) regardless of its
location with respect to ah line (vibrating line).
DISCUSSION:
There is more advancement in the field of dentistry including implants which increase a lot of retention in the prosthesis but still the need for physiologically retentive complete denture is there in developing countries like Pakistan1. Therefore, useful and precise treatment of
edentulous patients in the form of a retentive and functionally efficient complete denture is inevitable. So different techniques to enhance retention in complete denture including AH sound method, palpatory method, swallowing method and nose blowing method i.e Valsalva maneuver is used.2 In these techniques ah sound method is the easiest and mostly used by dental colleges and institutions.7,10,12 Previously
various studies have been done for finding the location of the vibrating line and fovea palatinae. TL LYE conducted a study with a sample size of 100 patients and found that radiographic, clinical, and histological studies indicate the location of the fovea palatinae was 1.31mm in front of the vibrating line. Out of 100 patients, fovea palatinae was visible in 92 patients. The patients who have fovea palatinae posterior to vibrating line were 12, 16 patients have fovea palatinae on vibrating line and 64 patients have fovea palatinae anterior to vibrating line. Our study also shows these type of results as in our study the patients have fovea palatinae anterior to vibrating line, posterior to vibrating line and also at vibrating line. Most of patients had fovea palatinae anterior to ah line that is single vibrating line. Silverman describes
that the posterior palatal seal could be extended 8.2 mm further dorsally to increase retention and stability. The vibrating line and fovea palatinae determines the extent of posterior palatal seal area. For good retention the posterior palatal seal should be in compressible soft tissue so that maxillary denture become retentive and sealed at post dam area. Here the soft palate type consideration is very important. In ClassI and Class II type soft palate there is expected wide compressible area of posterior palatal seal but in Class III always sharp margin of post dam is required as a little increase in size of posterior palatal seal can cause gagging , nausea and poor denture seal. Alaousi also conducted a study on 200 subjects and concluded that fovea palatine is a very important posterior palatal seal landmark that aids in denture retention. He selected patients randomly without inclusive criteria of soft palate type. In his study 50.9% of patients had their fovea palatinae and vibrating line coinciding, 44.5% of patients had vibrating line in front to the fovea palatinae and only 6.4% had vibrating line posterior to the fovea palatinae. Chen et al. also carried out a study on 104 subjects. Out of which 72 have visible fovea palatine. 25 % have coinciding fovea palatine and vibrating line and 75% have vibrating line anterior to fovea palatine but these results have less coincidence with our study as our subjects show more subjects with fovea palatine anterior to vibrating line and fewer subjects have fovea palatine posterior to vibrating
line. We also suggest a single ah line that is vibrating line concept, it is more reliable than confusion between anterior and posterior ah line or vibrating line concept. As it is demarcated in patients when they pronounce ah in short vigorous bursts. Fenn and associates and Anderson and Storer defined fovea palatine in the glandular region of the soft palate. Sears and Nagle suggest the fovea palatine mark the posterior limit of the hard palate and Sicher suggests the fovea palatine is present immediately behind the boundary of the hard and soft palate junction. Swenson suggests that the vibrating line is 2mm anterior to the fovea palatine
CONCLUSION:
The location of the fovea palatine is of utmost importancevduring forming the posterior palatal seal in the maxillary denture. Its location helps the dentist in creating an adequate seal of the maxillary denture by pressing the soft tissue. The exact location and demarcation of fovea palatine and ah line whether fovea is anterior, posterior or at ah line i.e. vibrating line provides an ideal guide for the posterior palatal seal of the maxillary denture.
CONFLICT OF INTEREST:
None declared
REFERENCES:
1. Kumar B, Naz A, Rashid H, Butt AM. Location of the Vibrating Line with Respect to Fovea Palatini in Class I, Class II and Class III
Soft Palate Types. J Pak Dent Assoc. 2016;25:60-66.
2. Zarb G, Hobkirk JA, Eckert SE, Jacob RF. Prosthodontic treatment for edentulous patients. (13th Ed.) St. Louis: Elsevier
Mosby. 2013:176-252.
3. Krysinski ZJ, Prylinski M. Carving of a master cast to obtain a posterior palatal seal of a complete maxillary denture as performed
by four prosthodontists: A pilot study. J Oral Sci. 2007;49:129-32.
https://doi.org/10.2334/josnusd.49.129
4. Yasmen T. Reliability of fovea palatinea in determining the posterior palatal seal. J Baghdad Coll Dent. 2009;21:41-55.
5. Sanofer AA, Gounder R. Assessment of the location of fovea palatine in relation to vibrating line in South Indian population. J Int Dent Med Res. 2017;10:883-6.
6. Goyal S, Goyal MK, Balkrishanan D, Hegde V, Narayana AI. The posterior palatal seal: Its rationale and importance: An overview. Eur
J Prosthodont. 2014;2:41-7.
https://doi.org/10.4103/2347-4610.131972
7. Kyung KY, Kim KD, Jung BY. The study of anatomic structures in establishing the posterior seal area for maxillary complete dentures.
J Prosthet Dent. 2014;112:494-500.
https://doi.org/10.1016/j.prosdent.2014.01.002
8. Lye TL. The significance of the fovea palatini in complete denture prosthodontics. J Prosthet Dent. 1975;33:504-10.
https://doi.org/10.1016/S0022-3913(75)80162-4
9. Akhtar N, Tanveer S, Chaudhary MA, Ahmad S. The reliability of foveae palatinae in determining the location of vibrating line in
edentulous patients. Pak Oral Dent J. 2017; 37:368-70.
10. Limbu IK, Basnet BB. Relationship of fovea palatinae to vibrating line as a reliable guide in determining the posterior limit of maxillary
denture. J Oral Res Review. 2019;11:68.
https://doi.org/10.4103/jorr.jorr_1_19
11. Thapa D, Chandra S, Karki S. Verifying relationship between fovea palatini, vibrating lines and junction between hard and soft palate.
Orthodontic J Nepal. 2016;6:32-4.
https://doi.org/10.3126/ojn.v6i1.16177
12. Hussain SZ, Samejo I, Qamar K. An investigation in to the concepts and techniques used for establishing postpalatal seal in undergraduate dental curriculum. Pak Oral Dent J. 2010;30.
13. Kumar B, Rameez M, Rashid H. Methods used to establish the posterior palatal seal for maxillary complete denture prosthesis. The
Pak J Medicine Dentistry. 2019;8:6-.
14. Ferro KJ, Morgano SM, Driscoll CF, Freilich MA, Guckes AD, Knoernschild KL, McGarry TJ, Twain M. The Glossary of Prosthodontic
Terms.
15. Mishra S, Rashmi BM, Ravishankar K, Khan S, Sharma A, Midhula V. Contemporary concepts and techniques of teaching posterior palatal seal among dental colleges of karnataka: a cross-sectional survey. J Clin Diag Res. 2020;14.
https://doi.org/10.7860/JCDR/2020/43743.14006
16. Lekay-Adams MR. A comparison of posterior palatal seal creation in complete dentures by private practitioners and students at the
University of Pretoria (Doctoral dissertation, University of Pretoria).
17. Chhetri S, Rathi A, Gupta N. Relation of fovea palatine and vibrating line in different soft palatal forms. J Nobel Med Coll. 2019;8:12-5.
https://doi.org/10.3126/jonmc.v8i1.24449
18. Maller SV. arthi KS. A review posterior palatal seal. J Ind Acad Dent Spec. 2010;1:16-21.