
Correlation of Education Level with Severity of Gingivitis and Plaque Score
INTRODUCTION:
Oral health is an integral component of general health, negligence in it can lead to a variety of dental problems.1 Dental professionals counsel their patients for oral health care and regular oral hygiene maintenance. Oral hygiene is the practice of keeping the oral cavity clean and healthy. Oral health status is greatly influenced by oral hygiene habits which include tooth brushing, use of oral hygiene aids, proper dietary practice and routine dental visits.1
It prevents plaque buildup, calculus and stain formation on teeth.2 Plaque biofilm is a complex community of multiple microorganisms found on a tooth surface. It has been established through clinical studies and microbiological analysis that plaque has a major role in initiation and progression of gingival inflammation as well
as other oral diseases.3 This inflammation remain unresolved as long as this microbial biofilm of plaque is present.4
General and oral health are both affected by the social determinants which include education, poverty, gender and
sustainability as stated by Human Development Index report 2020.5 These determinants have an impact on oral hygiene practices.2 Educational status is an important indicator of the awareness and behavior of the people for oral health.6 Educated individuals tend to have more knowledge about oral diseases, their prevention and are more likely to attend preventive or follow-up visits. They have better oral health status than those individuals who have lower education levels.1 They also comply better with oral health care regimens.6 A study conducted on elderly population of Nigeria reported high scores of plaque index among the individuals with primary education.2 Longitudinal study with span of 32 years found association of education level with brushing habits and revealed high plaque scores among the individuals with low educational levels.7 Gingivitis has been defined as the reversible plaque induced inflammation of the gingiva without detectable bone loss or clinical attachment loss. Clinically it presents as
erythematous, sore, swollen and bleeding gums.8 It effects more than 75% of the population worldwide and is the second most common oral disease.4 Presence of dental plaque is strongly associated with the presence of gingival
inflammation.3 A study conducted among Saudi adult population showed that males who presented with excessive plaque accumulation showed more severe signs of gingival inflammation.4
Education level has a significant association with severity of gingivitis.9 A study conducted on adult male population in Nigeria reported higher prevalence of gingivitis among the participants with low educational level.10
Literature indicates a weak link of education status with oral hygiene and gingivitis, however direct correlation of
education status with plaque score and severity of gingivitis is still lacking. The present study was designed to find
correlation of plaque scores and severity of gingivitis in patients with different education levels reporting to
periodontology department at Islamabad Dental Hospital. To find correlation participants of groups were equally
distributed. A base line data from this study will help in identifying the current oral health status of local population
belonging to different education levels.
METHODOLOGY:
This cross-sectional study was conducted at the Periodontology department of Islamabad Dental Hospital
(IDH) from May 2018 to May 2019, after the approval from Institutional Review Board (IRB) (Ref# IMDC/DS/IRB/118). The sample size was calculated to be 91 per group with absolute precision of 0.1 and anticipated proportion for gingivitis as 0.62 at 95% confidence level. Therefore, the minimum total sample size was 364 which was inflated to 384 to manage any incorrect or insufficient data. Out of these 8 were excluded (2 from each group) due to incomplete information. The final sample included 376 patients (94 per group). Since there was no such study reporting the correlation of education level with severity of gingivitis therefore prevalence of gingivitis was used for sample size calculation. The study population included systemically healthy patients (excluding those who were diabetic, immunocompromised, receiving psychological treatment, suffering from metabolic disorders etc.) of age 23 and above, presenting with symptoms of gingivitis. Patients with compromised hand dexterity and those who have received scaling within last one month were also not included in the study.
After taking informed consent, socio demographic data and complete medical history was recorded. Intraoral examination was conducted for plaque and gingival scores. Participants were equally recruited into four educational
groups having 94 patients in each group. Educational groups were categorized as illiterate (no formal education), primary (grade 1-8), secondary (grade 9-12) and tertiary (with bachelor’s, master’s and doctoral degrees).
Each group was evaluated on basis of visible plaque index (VPI) and modified gingival index (MGI). Clinical
examination was carried out by two trained examiners. Interexaminer reliability for both the indices was calculated on 30 patients which was 80% for plaque index and 75% for modified gingival index. Absence (0) or presence (1) of
dental plaque was visually assessed according to Ainamo and Bay index and percentage was calculated. Educational
group was further divided into two subgroups for plaque index i.e., plaque < 30 % and > 30%. Modified Le -Silness
index was used for assessment of gingival status. Four surfaces (Disto-buccal, mid buccal, mesio-buccal and lingual)
were scored for each tooth except for third molars. For MGI index each educational group was further divided into three subgroups (mild, moderate and severe gingival inflammation) having scores of (0.1 -1.0), (1.1-2.0) and (2.1-3.0)
respectively.11 Percentages of mild, moderate and severe periodontitis were calculated for each group and spearman’s correlation test was applied to find out the relation of education level with plaque score and severity of gingivitis. Spearman’s correlation test was also applied to find the relation between VPI score and MGI score. P-value of <0.01 was considered significant at 95% confidence interval.
RESULTS:
Study sample consisted of 376 patients out of which 186 (49.5%) were females and 190 (50.5%) were males. Individuals of age 23 and above were included since the average age of graduation in Pakistan is 23 yrs. Majority
of males 53 (28.5%) had tertiary education, 52 (28%) were uneducated, while 56 (29.5%) females were educated till primary and 51 (27.4%) had secondary education. Regarding the severity of gingivitis, majority of females 136 (73.1%) had moderate inflammation. Higher percentage of males 46 (24.7%) showed severe gingival inflammation as compared to females 38 (20%). More males (58.1%) presented with VPI score > 30 as compared to females (54.7%).
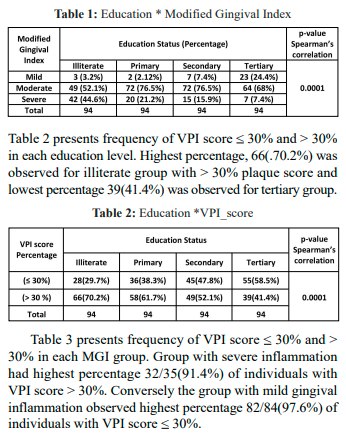
Table 1 shows the frequency of gingivitis by severity in groups of different education levels. Over all moderate
gingivitis was most prevalent. The illiterate group presented with the highest percentage 42 (44.6%) of severe gingivitis and lowest percentage 7 (7.4%) was observed in tertiary group. Similarly, highest percentage 23 (24.4%) of mild gingivitis was observed in tertiary group whereas primary and secondary groups presented with highest percentage 72(28%) of moderate gingivitia.
 A Spearman’s correlation of -0.2 (p-value<0.001) was observed for plaque score and -0.3 (p-value<0.001) was
A Spearman’s correlation of -0.2 (p-value<0.001) was observed for plaque score and -0.3 (p-value<0.001) was
observed for gingival index which is a fair correlation and implies that as the education level increased gingival and
plaque scores decreased.
The Spearman’s correlation between plaque score and gingival index also demonstrated a moderate, positive correlation (= 0.5, p-value< 0.001) which indicates that greater score of VPI corresponds to greater value of MGI score.
DISCUSSION:
Education plays a pivotal role in positive behavioral changes. In Pakistan as majority of the individuals belong
to primary education status,12 it is therefore, extremely important to inculcate dental health education in early years.
Education level has an impact on oral hygiene status.13 Present study concluded that lower level of education is
moderately co-related to poor oral hygiene with coefficient of -0.2 and a good relation was observed between poor oral hygiene and higher scores of gingival inflammation with coefficient of 0.5. Reports have shown that the participants with primary education and VPI > 30% presented with moderate gingival inflammation.14 A study carried out on Swiss Army recruits reported that individuals who completed 9 years of education presented with a mean plaque score of (1.41), whereas the university students merely showed a mean plaque score of (1.26) and the difference was statistically significant.15 Another study conducted on elderly reported that higher percentage of individuals who attended high school presented with acceptable plaque index as compared to those who didn’t attend high school.16 Lower educational status has been associated with lack of oral hygiene awareness resulting in higher levels of dental plaque, a primary etiological factor for development of gingival diseases.10,11
Gingival inflammation is a reversible condition and appropriate plaque control methods and professional dental
care can prevent disease progression.14 The results of present study also revealed higher scores of plaque among male subjects which coincide with the results of adults in Latin
America showing males with greater percentage of supragingival plaque sites than females.17 Ericsson JS et al
also reported that females had significantly lower level of dental plaque (41%) than males (53%).18
With regard to severity, moderate gingival inflammation (68.35%) was the most predominant type observed. Results of the current study are in agreement with those of previous reports that have documented high prevalence of moderate levels of disease.19 Regarding gender, men had higher MGI scores compared to women. According to international studies males presented with significantly higher frequency of severe gingivitis than did women.20,21 However, results of a cross sectional study revealed no statistical differences between genders when considering gingival inflammation which could be due to the overall low mean MGI score (1.2) for both groups.22
This study also reported a higher prevalence of gingivitis in individuals with low educational attainment with a moderate correlation of -0.3 which was statistically significant having p value of < 0.001. Some of the literature supports the present results, underscoring the relation of low education level with severe gingival inflammation.9,23,24
Most of the confounders in this study were controlled and all the educational groups had equal number of
participants, which is the strength of this study. Silness-Le plaque index and gingival index was not used which can
give us a better assessment of quantity of plaque buildup and gingival inflammation respectively. Brushing habits should also have been analyzed which could have given a clearer picture.
CONCLUSION:
It was concluded that participants belonging to low educational status presented with higher scores of plaque
and gingival index. Individuals with tertiary education presented with lower levels of plaque score and increased
prevalence of mild to moderate gingivitis. Females presented with better oral hygiene and gingival status than males.
Nearly two-third of the participants presented with moderate gingival inflammation.
RECOMMENDATIONS:
Under the light of the current results, it is prudent that the community based programs should include not only
dental education but also oral hygiene related workshops in early school years. It is necessary to increase the capacity
of these programs to the far reached areas where education level is low.
CONFLICT OF INTEREST:
None declared
REFERENCES:
1. Bonfim Mde L, Mattos FF, Ferreira e Ferreira E, Campos AC, Vargas AM. Social determinants of health and periodontal disease in Brazilian adults: a cross-sectional study. BMC Oral Health. 2013;13:22.
https://doi.org/10.1186/1472-6831-13-22
2. Braimoh O, Soroye M. Oral hygiene status of elderly population in Port Harcourt, Rivers State, Nigeria. African J Medical and Health Sciences. 2017;16:109-14.
https://doi.org/10.4103/ajmhs.ajmhs_39_17
3. Sreenivasan PK, Prasad KV. Distribution of dental plaque and gingivitis within the dental arches. J Int Med Res. 2017;45:1585-96.
https://doi.org/10.1177/0300060517705476
4. Idrees MM, Azzeghaiby SN, Hammad MM, ., Kujan OB. Prevalence and severity of plaque-induced gingivitis in a Saudi adult population. .35:1373-7. Saudi Med J. 2014;35:1373-7.
5. Conceição P, Jacob Assa, Cecilia Calderon, Fernanda Pavez Esbry, Ricardo Fuentes, Yu-Chieh Hsu, et al. The Next Frontier: Human development and the anthropocene. United Nations; 2020.
6. Kapoor D, Gill S, Singh A, Kaur I, Kapoor P. Oral hygiene awareness and practice amongst patients visiting the Department of Periodontology at a Dental College and Hospital in North India. Indian J Dent. 2014;5:64-8.
https://doi.org/10.4103/0975-962X.135262
7. Broadbent JM, Thomson WM, Boyens JV, Poulton R. Dental plaque and oral health during the first 32 years of life. J Am Dent Assoc. 2011;142:415-26.
https://doi.org/10.14219/jada.archive.2011.0197
8. Chrysanthakopoulos NA. Prevalence of gingivitis and associated factors in 13-16-year-old adolescents in Greece. European J Gen Dent. 2016;40:58-64.
https://doi.org/10.4103/2278-9626.179536
9. Sreenivasan PK, Prasad KVV, Javali SB. Oral health practices and prevalence of dental plaque and gingivitis among Indian adults. Clin Exp Dent Res. 2016;2:6-17.
https://doi.org/10.1002/cre2.15
10. Umoh AO, Azodo CC. Prevalence of gingivitis and periodontitis in an adult male population in Nigeria. ;9:65-9. Niger J Basic Clin Sci. 2012;9:65=9.
https://doi.org/10.4103/0331-8540.108465
11. Carvajal P, Gomez M, Gomes S, Costa R, Toledo A, Solanes F, et al. Prevalence, severity, and risk indicators of gingival inflammation in a multi-center study on South American adults: a cross sectional study. J Appl Oral Sci. 2016;24:524-34.
https://doi.org/10.1590/1678-775720160178
12. Shah D, Khan MI, Yaseen M, Kakli MB, Piracha ZF, Zia MA, et al. Pakistan Education Statistics 2017-18: NEMIS-AEPAM; 2021.
13. Umoh AO, Azodo CC. Association between periodontal Status, oral Hygiene status and tooth wear among adult male population in Benin city, Nigeria. Ann Med Health Sci Res. 2013;3:149-54.
https://doi.org/10.4103/2141-9248.113652
14. Elias-Boneta AR, Toro MJ, Rivas-Tumanyan S, Rajendra-Santosh AB, Brache M, Collins CJ. Prevalence, Severity, and Risk Factors of Gingival Inflammation in Caribbean Adults: A Multi-City, CrossSectional Study. P R Health Sci J. 2018;37:115-23.
15. Rothlisberger B, Kuonen P, Salvi GE, Gerber J, Pjetursson BE, Attstrom R, et al. Periodontal conditions in Swiss army recruits: a comparative study between the years 1985, 1996 and 2006. J Clin Periodontol. 2007;34:860-6.
https://doi.org/10.1111/j.1600-051X.2007.01124.x
16. Lacerda TeSP. Factors Associated With the Presence of Dental Plaque in an Urban Cohort of Elderly (Epidoso). MOJ Gerontology & Geriatrics. 2017;1:68-72.
https://doi.org/10.15406/mojgg.2017.01.00014
17. Oppermann RV, Haas AN, Rosing CK, Susin C. Epidemiology of periodontal diseases in adults from Latin America. Periodontol 2000. 2015;67:13-33.
https://doi.org/10.1111/prd.12061
18. Ericsson JS, Ostberg AL, Wennstrom JL, Abrahamsson KH. Oral health-related perceptions, attitudes, and behavior in relation to oral hygiene conditions in an adolescent population. Eur J Oral Sci.2012;120:335-41.
https://doi.org/10.1111/j.1600-0722.2012.00970.x
19. Murillo G, Vargas MA, Castillo J, Serrano JJ, Ramirez GM. Prevalence and severity of plaque-induced gingivitis in three Latin American cities: Mexico City-Mexico, Great Metropolitan Area-Costa Rica and Bogota-Colombia. Odovtos. Int J Dent Sc. 2018;20:91-102.
https://doi.org/10.15517/ijds.v20i2.32451
20. Mostafa B, El-Refai I. Prevalence of Plaque-Induced Gingivitis in a Sample of the Adult Egyptian Population. Open Access Maced J Med Sci. 2018;6:554-8.
https://doi.org/10.3889/oamjms.2018.131
21. Elias-Boneta AR, Encarnacion A, Rivas-Tumanyan S, BerriosOuslan BC, Garcia-Godoy B, Murillo M, et al. Prevalence of Gingivitis in a Group of 35- to 70-Year-Olds Residing in Puerto Rico. P R Health Sci J. 2017;36:140-5.
22. Jordan RA, Lucaciu A, Fotouhi K, Markovic L, Gaengler P, Zimmer S. Pilot pathfinder survey of oral hygiene and periodontal conditions in the rural population of The Gambia (West Africa). Int J Dent Hyg.
2011;9:53-9.
https://doi.org/10.1111/j.1601-5037.2009.00435.x
23. Australian Research Centre for Population Oral Health TUoASA. Periodontal diseases in the Australian adult population. Aust Dent J. 2009;54:390-3.
https://doi.org/10.1111/j.1834-7819.2009.01167.x
24. Ababneh KT, Abu Hwaij ZM, Khader YS. Prevalence and risk indicators of gingivitis and periodontitis in a multi-centre study in North Jordan: a cross sectional study. BMC Oral Health. 2012;12:1.
https://doi.org/10.1186/1472-6831-12-1