
Knowledge Regarding Prescription of Antibiotic for Endodontic Treatment among House Officers of Multan
INTRODUCTION:
Anti-microbials have been commonly used in the treatment of odontogenic diseases since their discovery. Anti-infection medication were
introduced, which led to a dramatic drop in the occurrence of dangerous contaminations and foreshadowing a remarkable phase in the treatment of incurable diseases.1 Medication treatment has been the primary tool applied by medical care professionals to enhance the patient’s wellbeing. Prescribing a drug is a dynamic & individualized clinical process.2,3 Since last decade, micro-organism’s evolutionary responses to the particular pressure wielded  by the antibiotics have led to resistant of microbial species against nearly each identified antibiotic agent. Antibiotic abuse and overuse have been implicated as major contributors to the emergence of multidrug-resistant strains.4,5 Antibiotic resistance is increasing in obligatory anaerobic bacteria, with clindamycin, cephalosporin, and penicillin resistance discovered in both major and small hospitals6. Before administering antibiotics, the benefit-to-risk ratio should always be considered. Certain patients will benefit from antibiotics, particularly those delivered systemically. In endodontic clinical therapy, antibiotics should be administered conservatively and judiciously; nonetheless, indiscriminate use (patients with pulpitis but no infection) is against basic medical practices. This could lead to a selective pressure and an increase of naturally hardy bacteria, exposing people to super and secondary infections and rendering therapies ineffective against potentially fatal infectious diseases.7,1
Prescription is a dynamic, customized clinical process, which is set owing to the necessities of patient & the acquaintance of the practitioner.8 Prescription writing is considered as necessary determinant of a medical or dental practitioner and has been part of the syllabus during their graduation.9 It is also an obligatory skill for doctors of all specialities.10
Dentists prescribe various drugs for a number of situations. If these medications are not recommended accordingly, they might cause damage to patient. Adverse medication events are stated to have been linked withmistake or incorrect writing of the prescription.11,12 Even if none of these instances end in death, they may induce morbidity in a certain individual. The act of suggesting has gotten increasingly difficult in recent years for a variety of reasons.
Prescription mistakes are classified into two types: prescription writing errors and decision-making errors. While the latter may consist of errors, such as overprescribing, under prescribing, inappropriate prescribingand irrational prescribingwhilethe formeremphases on errors made during writing of a prescription.13,14 Several studies have found poor prescription by students and junior practitioners, with some of the blame being assigned to knowledge or information-based errors.15,16 The goal of this study was to assess and evaluate house officers’ expertise of providing antibiotics for root canal therapy, as well as the errors they made.
METHODOLOGY:
Forty Multan Dental College house officers took part in this survey-based study. A survey form was developed to collect information on the reasons for prescribing antibiotics as well as the circumstances in which House officials recommended them. To collect data, the universal sampling approach was utilized. The questionnaire assessed house officers’ understanding of antibiotic prescription indications for a wide range of clinical symptoms associated with oral cavity infections. Malaise and fever were clinical markers, as were scattered edoema, indications of systemic spread, and swallowing difficulties. Participants were also asked if they had any clinical cases in which antibiotics were required, as well as what therapy they favoured, if any. Acute apical abscess, acute pulpitis, chronic apical periodontitis, and long-term apical swelling with sinus tract were the clinical situations studied. Factors influencing antibiotic prescriptions were also explored. The questionnaire asked if the patient’s expectation of receiving an antibiotic, multiple visit root canal procedures, single visit RCT, or retreatment may be the reason for the antibiotics being prescribed. The second section of the questionnaire assessed/evaluated knowledge of medical circumstances and oral procedures that may require prophylactic antibiotics. The oral procedures were all randomized controlled trials, including pre and post endodontic surgeries; the medical conditions included hepatitis B, HIV, congenital heart diseases, mitral valve prolapsed, uncontrolled diabetes, and patients who had prosthetic joints in the previous two years or those reporting a history of radiotherapy and cancer. The data obtained was collated and examined.
RESULTS:
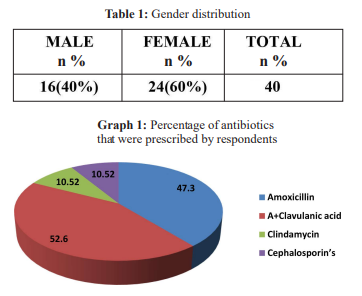
This study included 24 females and 16 males (Table 1). The most incidence of antibiotic prescription was reported for acute abscess of periapical area of the tooth (62.8%) and patient having fever with malaise (62%). Antibiotic prescription for Chronic apical abscess and Chronic periodontitis with sinus tract is 58%. and 55% respectively
Patients with swelling & difficulty in swallowing (58%) while 33% was reported during prolong root canal treatment. Overall, 12% of partakers always suggested antibiotics for root canal treatment.
In the study mostly antibiotics were prescribed as prophylactic measures for congenital heart diseases 69.7%, and 62.8% is for poorly controlled diabetes mellitus. Participants prescribed Prosthetic joint in past 2 years 4 6.5% & Mitral valve prolapsed 34.9%. Graph 2

DISCUSSION:
The majority of oral issues are inflammatory conditions that produce pain. In many cases, chronic or acute infections of the pulp produce oral pain, needing surgical surgery rather than medications. Antibiotics are not always required to treat endodontic source problems1.Amoxicillin + clavulanic acid (52.6%) and Amoxicillin alone (47.3%) were the drugs of choice in this study, which is similar to other studies in which Amoxicillin was the medicine of choice 57.6% & 46.47% 17,18. Clindamycin was usually the last choice in this study. These findings are congruent with those of Fahad et al and Jain A et al, who discovered that amoxicillin was the most often suggested antibiotic, whereas clindamycin was rarely used.19,18
Antibiotics were predominantly administered for acute apical abscess (62.8%) in our study, which differs with the findings of M Reza et al, who utilised antibiotics for apical/dental abscess (74% & 71%, respectively).17,19 This finding is similar with another study20, which found that antibiotics were given to 62.6% of participants with peri-apical abscess. Our survey found that 62% of patients with malaise and fever were given antibiotics, which is similar to another study that found that 57% of patients with fever were given antibiotics.19 In this investigation, 25.5% contributors suggested antibiotics for acute pulpal inflammation which is twofold as reported by Palmer et al where 12.5% of participants advised antibiotics for acute pulpitis21 and this is three fold as compared to another study (8.2%).20 Antibiotics may not be needed and may not help critical pulp situations when there are no symptoms of systemic or local involvement/infection22, in contrast to the current study in which antibiotics were taken for pulpal disorders by the majority of individuals.
Debridement of the root canal space is the recommended therapy for irreversible pulpitis. Non-surgical root canal treatment without antibiotics is often sufficient to treat chronic apical periodontitis, acute pulpitis, irreversible pulpitis, and draining sinus area. The pulpal circulation/flow is frequently disrupted in these situations, and systemic antibiotics may not reach the required therapeutic concentrations inside the pulp.23 A thorough non-surgical root canal treatment might eradicate the source of the infection and typically allow healing of the peri-radicular lesion. Nonetheless, analgesics are used for  peri-apical diseases and pulpitis pain.17
58% of partakers of this study specified the use of antibiotics in Chronic apical abscess with sinus tract which is two times that of reported in another study.55% of partakers of this study specified the use of antibiotics in Chronic apical abscess with periodontitis which is far greater than that reported in another study.24 Results of this study stated that 33% participants give antibiotics during the root canal treatment which is like the result of other study where 35.2% partakers wrote antibiotics during RCT.20 About 11.6% of defendants used to recommend antibiotics afterward root channel treatment. For peri-apical chronic lesions and chronic peri-apical abscess with sinus tracts, fifty eight percent & fifty five percent respondents recommendedan antibiotic respectively which is similar to the results stated by Nabavezadeh et al(58% and 73.1%) respectively.14 Our study showed that 55% subjects gave antibiotics apical abscess with periodontitis which is like the result of other study where 58% partakers wrote antibiotics as an adjunct.19
13.9% participants of this study advice medicine before RCT which is quite similar to another study which indicates 11.4%. 41.9% participants of this study advice antibiotics for HIV+ patients. This is in accordance with the other study where 58% of dentists stated prescribing antibiotics. In the current study, 25.6% of patients with a history of carcinoma and chemo/radiotherapy were prescribed antibiotics. This figure is lower than that reported by Yousufi S (40.6%).20 Our
study found that 69.7% of individuals were given preventive antibiotics for congenital heart disease, which is somewhathigher than the number reported in another study, which was 6019. 34.9% participants reported that we prescribe prophylactic
antibiotics for mitral valve prolapsed patients which is alike with the study conducted by Fahad et al who reported 35%19. 14% subjects reported that they gave antibiotics if patients insist which is less than observed by Liaquat A et al (70%).25
Prophylactic antibiotic treatment is recommended only for patients who are at high risk of developing infective endocarditis following bacteremia. The use of prophylactic
antibiotics by these patients prevents blood-borne microorganisms from colonising shunts and prostheses or
spreading within a compromised system. Prophylactic antibiotics are required for patients with prosthetic mitral valve prolapses, uncontrolled diabetes, and inherited heart conditions (AV shunt and cardiac valve replacement) during endodontic  treatment1. Although antibiotic prophylaxis prior to endodontic therapy is not routinely recommended for healthy patients following prosthetic joint replacement, it should be considered during the first three months after the joint replacement.26,27
According to our current study, house officers at Multan Dental College use antibiotics improperly, which can lead to issues such as resistant microorganisms, drug resistance, and other negative results. This examination resulted that knowledge for the use of antibiotics is far from ideal. This was also reported in the Wali A study.28
In endodontics, the routine uses of antibiotics either systemic or local, is still a debatable issue.29 According to one study, dentists must administrate the antibiotics according to the guidelines, only if therapies or treatments require it.30 Antibiotic abuse is a major worldwide issue.31 Prescriptions must be logical and supported by extensive evidence-based knowledge. Medical and dental students, as well as healthcare workers, must be aware of the various aspects of the drugs prescribed in order to effectively treat the illness for which the drug was prescribed.32 According to evidence33, antibiotics may provide both benefits and harm in certain situations. Antibiotics, particularly broad-spectrum antibiotics, are commonly used in dentistry.34 Many studies on antibiotic prescription in dentistry have found that overuse is a global problem.35 Antibiotics may be used more frequently in endodontics.36 The publication of recommending protocols and guidelines may help to achieve better results, and appropriate educational intervention may also be effective. The use of computers and clinical audits, as well as additional tools to increase antibiotic prescription knowledge and improve and increased patient care, should always be considered.
CONCLUSION:
We conclude that here is deficiency of information & knowledge for the proper indication, kind, and antibiotics dose. Different educational activity like symposium or lectures should be practiced to teach the practitioner to prescribe antibiotics. The curriculum and syllabus should place a strong focus on prescribing, and appropriate medication prescription should be learnt through clinical rotations utilizing hypothetical or actual instances.
LIMITATIONS:
Sample size is very small. Multiple institutes were not included in the study. Different institutes delivered different level of knowledge to the students. Public institutes must be included in the future studies. Level of house officers were not mentioned in the study because as experience of the house officers’ increases, level of education must increase.
CONFLICT OF INTEREST:
None declared
REFERENCES:
1. Hargraeves KM, Cohen S, Burmen LH. Cohen’s Pathways of the Pulp 10thedition. Elsevier.2011
2. Rauniar GP, Roy RK, Das BP, Bhandari G, Bhattacharya SK. Prescription Writing Skills of Pre-Clinical Medical and Dental Undergraduate Students. J Nepal Med Assoc. 2008; 47:197-200.
https://doi.org/10.31729/jnma.157
3. Guzmán-Ãlvarez R, Medeiros M, Reyes Lagunes LI, CamposSepúlveda AE. Knowledge of drug prescription in dentistry students. Drug, Healthcare and Patient Safety. 2012; 4:55-9.
https://doi.org/10.2147/DHPS.S30984
4. Patel R: Clinical impact of vancomycin-resistant enterococci. J Antimicrob Chemother 51(Suppl 3):13, 2003.
https://doi.org/10.1093/jac/dkg272
5. Puttaswamy S, Gupta SK, Regunath H, Smith LP, Sengupta S. A comprehensive review of the present and future antibiotic susceptibility testing (AST) systems. Arch ClinMicrobiol. 2018;9.
https://doi.org/10.4172/1989-8436.100083
6. Fair RJ, Tor Y. Antibiotics and bacterial resistance in the 21st century. Perspectives in medicinal chemistry. 2014;6: PMC-S14459. 25-64
https://doi.org/10.4137/PMC.S14459
7. CDC. Antibiotic Use in the United States, 2017: Progress and Opportunities. Atlanta, GA: US Department of Health and Human Services, CDC; 2017.
8. Ashraf H, Pasha M, Nayyer M, Aslam A, Kaleem M. Drug Prescription Among Dental Students: A Survey of Current Knowledge and Awareness. Pak Oral Dent J. 2018;38:503-7
9. Parihar A, Sharma A, Malhotra P, Sharma D. Assessment of Prescription Writing Skills Among Undergraduates of a Medical College in North India. JK Science. 2018;20:67-72
10. Mahmood A, Tahir MW, Abid AN, Ullah MS, Sajjid M. Knowledge of drug prescription in dental students of Punjab Pakistan. Pakistan J Medi
Health Sci. 201812: 232- 7.
11. Tariq RA, Vashisht R, Scherbak Y. Medication errors. Stat Pearls [Internet]. 2020 Jun 15.
12. Lee BH. Minimizing prescription writing errors: Computerized prescription order entry. John Hopkins Medical Institutions 2006;1-10.
13. Alanazi MA, Tully MP, Lewis PJ. Prescribing errors by junior doctorsA comparison of errors with high risk medicines and non-high-risk medicines. PloS one. 2019;14: e0211270.
https://doi.org/10.1371/journal.pone.0211270
14. Aronson JK. Medication errors: definitions and classification. Br J Clin Phar. 2009;67:599-604.
https://doi.org/10.1111/j.1365-2125.2009.03415.x
15. Harding S, Nicky B, David B. The performance of junior doctors in applying cl inical pharmacology knowledge and prescribing skills to standardized clinical cases. Br J Clin Phar 2010;69:598-606.
https://doi.org/10.1111/j.1365-2125.2010.03645.x
16. Ross S, Bond C, Rothnie H, et al. What is the scale of prescribing errors committed by junior doctors? A systematic review. Br J Clin Phar 2008;67:629-40.
https://doi.org/10.1111/j.1365-2125.2008.03330.x
17. Nabavizadeh MR, Sahebi S, Nadian I. Antibiotic Prescription for Endodontic Treatment: General Dentist Knowledge + Practice in Shiraz. Iran Endod J 2011;6:54-59
18. Jain A, Gupta D, Singh D, Garg Y, Saxena A, Chaudhary H, et al. Knowledge regarding prescription of drugs among dental students: A descriptive study. J basic and clinical pharmacy. 2015 ;7:12.
https://doi.org/10.4103/0976-0105.170584
19. Ismail F, Qazia S, Sajjada A. Antibiotics Prescription Habits and Knowledge of Dentists in A Lahore Sample. Pak Oral Dent J. 2018;38:79- 84.
20. Yousufi S, Israr Y, Zaman S. Use of Antibiotics in Dental Teaching Hospitals of Peshawar, Pakistan: How Justified Are We. Int J Dent Oral Health. 2019; 5:68-73.
21. Palmer NA, Dailey YM, Martin MV. Can audit improve antibiotic prescribing in general dental practice? Br Dent J 2001; 191:253-5. https://doi.org/10.1038/sj.bdj.4801156a
22. Walton R: Endodontic Emergencies and Therapeutics. In: Torabinejad M, Walton R, editors. Endodontics principles and Practice, 4th Edition. St. louis: CV Saunders, 2009:153-4.
23. Segura-Egea JJ, Gould K, Sen BH, Jonasson P, Cotti E, Mazzoni A, et al. Antibiotics in Endodontics: a review. Int Endodontic J 2017;50:1169- 84.
https://doi.org/10.1111/iej.12741
24. Salvadori M, Audino E, Venturi G, Garo ML, Salgarello S. Antibiotic prescribing for endodontic infections: a survey of dental students in Italy. Int Endodontic J. 2019;52:1388-96.
https://doi.org/10.1111/iej.13126
25. Liaquat A, RCSI F, Tayyab TF, Saeed T. Are Dentists Prescribing the Antibiotics in Justified Conditions? An Exploratory Study. JPDA. 2020;29:120-123.
https://doi.org/10.25301/JPDA.293.120
26. Segura-Egea JJ, Gould K, Sen BH, Jonasson P, Cotti E, Mazzoni A, et al. European Society of Endodontology position statement: the use of
antibiotics in endodontics. Int Endodontic J. 2018;51:20-5.
https://doi.org/10.1111/iej.12781
27. Sollecito TP, Abt E, Lockhart PB, Truelove E, Paumier TM, Tracy SL, et al. The use of prophylactic antibiotics prior to dental procedures in patients with prosthetic joints: evidence-based clinical practice guideline for dental practitioners-a report of the American Dental Association Council on Scientific Affairs. J Am Dent Assoc. 2015;146:11-6.
https://doi.org/10.1016/j.adaj.2014.11.012
28. Wali A, Ali A, Siddiqui TM, Jafri H. Assessing prescription writing skills of House officers in Dental teaching hospitals of Karachi, Pakistan. World J Dent 2012;3:294 96
https://doi.org/10.5005/jp-journals-10015-1176
29. Nandakumar M, Nasim I. Use of Antibiotics in Endodontics-Clinical Practice Guidelines. Research J Pharmacy Technology. 2019;12:419-24.
https://doi.org/10.5958/0974-360X.2019.00076.3
30. Guerrini L, Monaco A, Pietropaoli D, Ortu E, Giannoni M, Marci MC. Antibiotics in dentistry: a narrative review of literature and guidelines considering antibiotic resistance. Open Dent J. 2019 ;13.
https://doi.org/10.2174/1874210601913010383
31. Iqbal MT, Ahmed MH, Omar N, Ahmed MR, Fahad M, Ali M, et al. Antibiotic Resistance: KAP Study on Medical and Non-Medical Students of Lahore, Pakistan. Pak J Public Health. 2020;10:24-31.
https://doi.org/10.32413/pjph.v10i1.504
32. Shahroom NS, Lakshmi T, Roy A. Knowledge of drug prescription among dental and medical student in India-an online survey. J Adv Pharm Educ Res|. 2017;7.
33. Lockhart, P.B., Tampi, M.P., Abt, E., Aminoshariae, A., Durkin, M.J., et al 2019. Evidence-based clinical practice guideline on antibiotic use for the urgent management of pulpal-and periapical-related dental pain and intraoral swelling: A report from the American Dental Association. J Am Dent Assoc, 150(11), pp.906-921.
https://doi.org/10.1016/j.adaj.2019.08.020
34. Anjum MS, Parthasarathi P, Monica M, Yadav K, Irram A, Keerthi T, et al. Evaluating the knowledge of interns in prescribing basic drugs used in dentistry-a cross-sectional study. Webmed Central Pharmacol 2014;5: WMC004540.
35. Teoh L, Marino RJ, Stewart K, McCullough MJ. A survey of prescribing practices by general dentists in Australia. BMC Oral Health.
2019;19:1-8.
https://doi.org/10.1186/s12903-019-0882-6
36. Bansal R, Jain A, Goyal M, Singh T, Sood H, Malviya HS. Antibiotic abuse during endodontic treatment: A contributing factor to antibiotic resistance. J Family Medicine and Primary Care. 2019;8:3518-24
https://doi.org/10.4103/jfmpc.jfmpc_768_19