
Effect Of Covering Curing Tip With Multi Protective Layers On Vicker’s Hardness Of Different Composites
INTRODUCTION
In dentistry, light cured resin composite have been widely used as esthetic restorative material for anterior and posterior teeth1. Light-cured resins contain photoinitiators, which are activated by blue light to begin the polymerization process. The light must have sufficient intensity and must be of the correct wave length to activate the photo-initiator. It has been documented that the rapid development of light-curing units (LCUs) has found to be parallel with the advancement in dental resins2,3.
The minimum light intensity required to adequately cure 1.5 to 2 mm of composite resin is reportedly between 280 and 300 mw/cm2 as both the physical and biological properties of resin composites are affected by the degree of polymerization4,5. Inadequate curing of the composite may cause problems such as premature breakdown at the margins and staining of the restoration, dimensional instability, decreased biocompatibility of the resin and increased cytotoxicity6,8.
Dental clinics must maintain a high level of infection control, in order to protect both patients and the dentist. According to the guidelines of Centers for Disease Control and Prevention (CDC) for Infection Control in Dental Health-Care Settings, patient-care items are divided as critical, semi-critical, or non-critical depending upon the possible risk for infection related with their intentional use9. Caughman and others had reported that after clinical use contamination of light guides and LCU handles were found to be common3. Presently the most common method of maintaining sterility of the light guide are wiping the guide with a disinfectant, such as glutaraldehyde, after each patient; using autoclavable guides; using presterilized, single-use plastic guides; and translucent disposable barriers to cover the guide10-12. Unfortunately, when light guide tips are autoclaved it increases boiler scale from vaporized water and need repeated polishing to keep optimal intensity of light. Chemical sterilization necessitate up to 10 hours of immersion which is not always possible, and not all clinics have facility for vapor sterilization13.
Disposable barriers are suitable, non invasive and cost-effective way of avoiding contamination of the light guide as it prevents direct contact between the oral tissues and the light guide14. These barriers also reduce the risk of damaging the light guide during autoclaving or disinfection15,16. Among various infection control barriers, the plastic wrap (food wrap) is commonly used as it has the little effect on the LCU power density17. But, a thin single-layer of wrap have a tendency to tear easily while the handling of LCU, or by the sharp edges of the prepared cavity18. As a result, more than one layer of wrap for infection control barrier is used which could reduce the risk of cross infection19. Conversely, a multi-layer infection control barrier wrap reduced the light output of the LCUs and accordingly it affects the polymerization resulted in reduced micro-hardness of the composite restoration18.
However, earlier studies have concluded that the light intensity may reduce up to 35% when barriers are used. Warren and others found that four different types of barrier used on each of four different light guides all reduced light output. One barrier reduced the power density from the curing light up to110 mW/cm2 19,20. Cellophane wrapped around the light guide has been caused the least reduction in power density from the curing light12. Although these studies were useful, they may have produced deceptive results because a dental radiometer was used to measure light intensity. Many dental radiometers do not provide reliable measurements, they do not report wavelength, and they may not accurately measure light intensity3,21.
Leonard and others had found that the accuracy of dental radiometers varies by as much as 80% and were dependent on the diameter of the light guide. Unlike a dental radiometer, a laboratory-grade spectrometer connected to an integrating sphere that can capture and measure all light output from an LCU and provides a visual display of the spectral output. For these reasons, a laboratory-grade spectrometer or photo spectrometer should be used to measure power output from dental curing lights as well as to record their spectral outputs21.
As Barry and colleagues claimed that radiometric evaluation of LED light units tested did not satisfy manufacturers claims for minimum intensities however the spectral emission from the light source did meet manufacturer requirements; most of the studies had used radiometer while there are only few studies have been documented that used spectrometer, thus this lacking of usage helped in setting the objectives of current study. 22.
The objective of this study was to evaluate the effect of a multi-layer barrier on the micro-hardness of different composite resin cured with a light emitting diode (LED)unit (Mectron Starlight Pro-LED, intensity 1.200 mW/cm2, Italy) and also estimated the intensity of LED lights with different protective layers.
The hypothesis tested was that multi layers of infection control barriers would have a significant effect on the intensities of LED light and micro-hardness of the different composite resin.
METHODOLOGY
This experimental study was conducted at Department of Operative Dentistry, Dr. Ishrat-ul-Ebad Khan Institute of Oral Health Sciences, Dow University of Health Sciences, Karachi. Microhardness evaluation was carried out at the Department of Material Sciences, NED University, Karachi, from August 2014 to January 2015.
Materials used in the study included a Hybrid composite ValuxTM Plus (3M Dental Products, St. Paul, MN, USA) , Nano resin composite Filtek_Z350 (3M Dental Products, St. Paul, MN, USA) and nano ceramic composite CeramoX (Dentsply Caulk, Milford, DE, USA). Detailed descriptions of the material are given in Table I.
Specimen preparation
A polytetrafluoroethylene mold of 10 mm in diameter and 2 mm thick was placed on a substrate consisting of a polyethylene sheet covered glass slide. The mold was filled with the uncured paste of dental composite and enclosed with a mylar strip and glass slide and light pressure was applied. This method provided specimens with smooth top and bottom surfaces. The restoration material was cured using an LED curing lamp (Mectron Starlight Pro-LED, intensity 1000 mW/cm2, Italy) for 20 seconds. LED curing lamp was covered with one, two, f o u r , Table 1: Materials used in the present study and
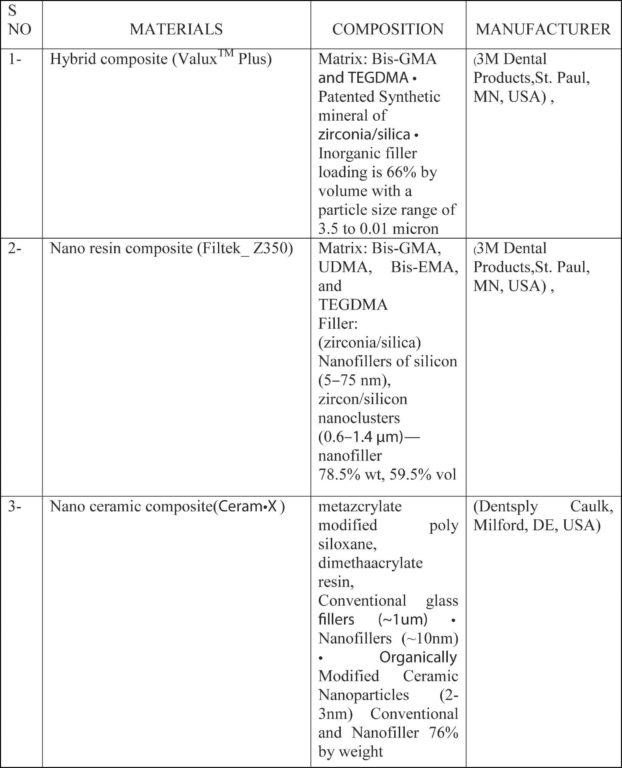
eight layers of a disposable wrap barrier (Cleanwrap,Gimhae, Korea). The thickness of single wrap barrier sheet is about 0.5 mils. The barrier was cut to an enough size and was used to cover the light guide without air entrapment; the specimens were matured in an incubator at 37 oC for 24 hours. Groups A1/B1/C1 (control) cured with LED covered with single wrap barrier, Groups A2/B2/C2 cured LED covered with two wrap barriers, Groups A3/B3/C3 cured LED covered with four wrap barriers led lamp, and Groups A4/B4/C4 cured Led covered with eight wrap barrier .
Micro hardness testing
Micro hardness of every specimen was determined using a micro-hardness tester (Micro-vickers hardness tester, Wolpert group, China) equipped with a diamond Vickers indenter. The indentation load was 100gm and the dwell time was 10 s. Three indentations spaced equally over the surface of each specimen.
Spectrophotometric Analysis
The spectral distribution generated by LCU with different number of plastic wrap was calculated by passing the light through a spectrophotometer model (Data color; SF 600; Plus-CT; USA). The unit was calibrated prior to wrapping. The tip of the light guide was placed over the aperture of an integrating sphere, which captured all light from the guide. The following 3 measurements were recorded: total power (mW), peak wavelength (nm) and irradiance at the peak value (mW/nm).The light output was measured with no barrier (control) and with each barrier.
The power recordings obtained from the spectrometer were converted into power density values (mW/cm2) by dividing the total power by the area of the tip of the light guide, since this is the unit in which values are commonly reported when LCUs are assessed.
Data were entered in IBM SPSS v. 21 (Chicago, Illinois, Inc.). Microhardness of different materials was presented in terms of mean and standard deviation. Two way Analysis of Variance (ANOVA) was used to compare micro hardness between groups and subgroups. Bonferroni (LSD) test was used to detect mean difference in each pair of groups. Tukey’s HSD test was used to observe significant difference between subgroups. Level of examining significant difference was kept atmost 0.05.
RESULTS
The data was analyzed for normal distribution prior to the use of multiple comparisons. The Q-Q plot analysis revealed a normal distribution of data, thus a parametric test ANOVA was utilized for statistical analysis. The mean micro hardness of micro hybrid composite (71.58± 3.51) was significantly less (p= .0000000051) than micro hardness of nano composite (82.63± 2.488) and nano ceram X (82.53±2.470). (Table 2 & 3).
Multiple comparisons between the control (single wrap) and multiple barrier method revealed statistically
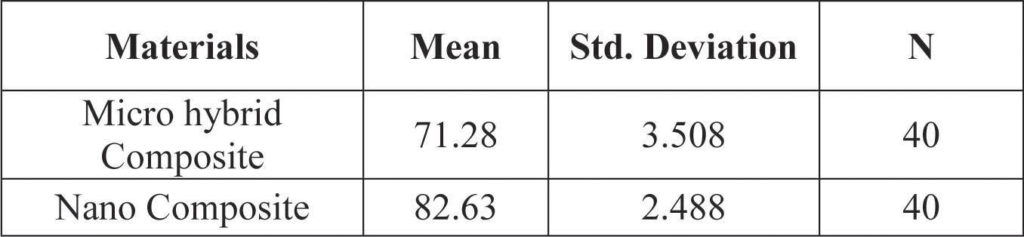 Table 2: Means (+ standard deviation) (Vickers) of the micro hardness values obtained for the of different type of composite
Table 2: Means (+ standard deviation) (Vickers) of the micro hardness values obtained for the of different type of composite
significant difference. Micro hardness of eight wrap micro-hybrid composite (A4) was significantly low than its other 3 counterparts (A1, A2, A3) (P < 0.0001). Similar
 Table 3: Means (±SD) and p values of Vickers Hardness
Table 3: Means (±SD) and p values of Vickers Hardness
results were observed for eight wrap subgroups of Nano composite (B4) and Nano Ceram (C4). (P Value = .0000015599 for B4, p= .0000290233 for C4) as shown in table III and graph no 1.
Spectrophotometric Analysis
 Graph no 1 Mean Plot
Graph no 1 Mean Plot
The mean values for the light intensity records for the control (single wrap) and Two Wrap, four wrap and eight wrap were 570 mW/cm2, 565.52 mW/cm2, 535.4mW/cm2, and 497.0mW/cm2, respectively.
DISCUSSION
 It is important that curing tips used for curing resin composites in the mouth must be sterile as well as it is also an essential aspect to ensure that the resin receives sufficient power density and appropriate spectral output for adequate curing. The current study has revealed that usage of eight layers for infection-control barriers reduces the intensity of LCU as evaluated by spectrophotometer, as well as micro-hardness of composites was also reduced. On the contrary, covering curing tip with up to four layers wrap did not show any considerable effect on power density and microhardness. It might be due to the fact that distance from the tip of the light guide to the resin has a much greater effect on power density. It has been reported that 1-mm space between the light guide and the resin may cause a reduction in power density of between 8% to 16%23. With increasing number of layers the distance of curing unit from restoration is also increased, thus decreasing the light intensity and adversely affect the cure and hardness of the composite resin24.
It is important that curing tips used for curing resin composites in the mouth must be sterile as well as it is also an essential aspect to ensure that the resin receives sufficient power density and appropriate spectral output for adequate curing. The current study has revealed that usage of eight layers for infection-control barriers reduces the intensity of LCU as evaluated by spectrophotometer, as well as micro-hardness of composites was also reduced. On the contrary, covering curing tip with up to four layers wrap did not show any considerable effect on power density and microhardness. It might be due to the fact that distance from the tip of the light guide to the resin has a much greater effect on power density. It has been reported that 1-mm space between the light guide and the resin may cause a reduction in power density of between 8% to 16%23. With increasing number of layers the distance of curing unit from restoration is also increased, thus decreasing the light intensity and adversely affect the cure and hardness of the composite resin24.
Light produced by light curing unit has a direct effect on the polymerization of restoration by the virtue of spectral emission and power intensity25. Diameter of a curing tip as well as shade of material altogether exert direct effect on light penetrance and eventually the hardness of restoration. In the present study we overcame this limitation by choosing single material of same shade and same light diameter in order to achieve uniform experimental conditions. Furthermore, hand held portable light meters have been used to check intensity of lights as they are relatively inexpensive and easy to use, however its consistency and accuracy has been challenged26. According to Barry and Rodriguez, evaluation of LED units tested by radiometer did not satisfy manufactures claim but spectral emission by Spectrophotometer did meet the manufacturer’s requirement. Thus, in this study we used spectrophotometer to overcome this
limitation22,27.Micro-hardness testing has been used in many previous researches, because surface hardness has been commonly correlated with physical properties of material like mechanical strength and shown to be an indicator of the degree of polymerization28,29. The null hypothesis of the current study was partially accepted and demonstrated that eight wrap has significantly reduced the micro-hardness of all type of tested composite. On the contrary, one, two and four wrap barrier did not significantly affect the hardness. These findings are in accordance to the study reported by Scott et al17.
Results of present study corroborate with the results of Chong et al. They concluded that increase in thickness of infection control barrier reduced the light output. In our study significant reduction in hardness were seen in all three materials when eight layer wrap were used because each layer thickness was about 0.5 mils and 8 wrap thickness was about 0.1016 mm.30
Al Marzok observed a reduction in light intensity on radio meter on using barriers of different thicknesses; however the hardness values were not affected. These results were not in concordance our findings because they had used knoop hardness test whereas, in our study Vicker’s hardness test was used, which is considered as better indicator of the degree of polymerization28.
When choosing a procedure to disinfect curing tips, dentist should consider numerous aspects. If the curing tips are to be autoclaved between patients, then it is necessary to purchase additional tips. Disposable Cure Sleeve barriers and Cure Elastic barriers are available and are expensive; but plastic wrap is the most cost effective and about 10 cm of plastic wrap is enough to cover a curing tip.
According to the results of this in vitro study, four layers rather than two layer of an infection control barrier should be used in order to decrease the possibility of cross infection and chance of easy tear with single or two layers. It is also recommended that several manufacturers have provided disposable, plastic infection control barriers as an effective mean of protection for both the unit as well as the curing tips. Although these barriers do not significantly affect spectral distribution, the irradiance is reduced, especially if the beam of the barrier lies across the light tip31.
This present study has some limitations as it could not completely replicate the complex oral environment.
The role of artificial saliva, thermo cycler and all versions of materials were not taken into consideration.
CONCLUSION
Within the limitations of this in vitro study, we conclude that wrapping the light-cure tip with one, two or four wrap has no significant effect on the micro hardness of the all types of cured composite resin. While the eight warp barrier significantly reduced the micro hardness of composite resin.
REFERENCES
- Kawaguchi M, Fukushima T, Miyazaki K. The relationship between cure depth and transmission coefficient of visible-light-activated resin composites. J Dent Res 1994;73:516-21.
- Anusavice KJ. Phillips’ science of dental materials.11th ed. St. Louis: Elsevier Science; 2003. p. 411.
- Rueggeberg FA. Precision of hand-held dental radiometers. Quintessence Int 1993;24:391-6.
- Forss H, Widstrom E. From amalgam to composite: selection of restorative materials and restoration longevity in Finland. Acta Odontol Scand 2001;59:57-62.
- Fan PL, Schumacher RM, Azzolin K, Geary R, Eichmiller FC. Curinglight intensity and depth of cure of resin-based composites tested according to international standards. J Am Dent Assoc 2002;133:429-34.
- Pearson GJ, Longman CM. Water sorption and solubility of resinbased materials following inadequate polymerization by a visible-light curing system. J Oral Rehab 1989; 16:57-61.
- Ferracane JL. Correlation between hardness and degree of conversion during the setting reaction of unfilled dental restorative resins. Dent Mater 1985; 1:11-14.
- Chen RS, Liuiw CC, Tseng WY, Hong CY, Hsieh CC, Jeng JH. The effect of curing light intensity on the cytotoxicity of a dentin-bonding agent. Oper Dent 2001; 26:505-510.
- Kohn WG, Collins AS, Cleveland JL, Harte JA, Eklund KJ, Malvitz DM. Guidelines for infection control in dental health-caresettings. MMWR Recomm Rep 2003;52:161.
- Rueggeberg FA, Caughman WF, Comer RW. The effect of autoclaving on energy transmission through light-curing tips. J Am Dent Assoc 1996; 127(8):11831187.
- Rueggeberg FA, Caughman WF. Factors affecting light transmission of single-use, plastic light-curing tips. Oper Dent 1998; 23:179-184.
- Chong SL, Lam YK, Lee FK, Ramalingam L, YeoAC, Lim CC. Effect of various infection-control methods for light-cure units on the cure of composite resins. Oper Dent 1998; 23(3):150-154.
- Kakaboura A, Tzoutzas J, Pitsinigos D, Vougiouklakis G. The effect of sterilization methods on the light transmissioncharacteristics and structure of light-curing tips. J Oral Rehabil. 2004;31:918-923.
- Chang HS. Infection control of light curing units. J Korean Acad Conserv Dent 2010;35:235-237.
- McAndrew R, Lynch CD, Pavli M, Bannon A, Milward P. The effect of disposable infection control barriers and physical damage on the power output of light curing units and light curing tips. Br Dent J 2011;210:E12.
- Pollington S, Kahakachchi N, van Noort R. The influence of plastic light cure sheaths on the hardness of composite resin. Oper Dent. 2009;34:741-745.
- Scott BA, Felix CA, Price RB. Effect of disposable infection control barriers on light output from dental curing lights. J CanDent Assoc 2004;70:105-110.
- Chang HS, Lee SR, Hong SO, Ryu HW, Song CK, Min KS. Effect of infection control barrier thickness on light curing units. J Korean Acad Conserv Dent 2010;35:368-373.
- Miller CH, Palenik CJ. Infection control and management of hazardous materials. St. Louis: Mosby Pub. Co.; 1994.
- Warren DP, Rice HC, Powers JM. Intensity of curing lights affected by barriers. J Dent Hyg 2000;74:20-23.
- Leonard DL, Charlton DG, Roberts HW, Cohen ME. Polymerization efficiency of LED curing lights. J Esthet Restore Dent 2002;14:286-295.
- Owens BM, Rodriguez KH. Radiometeric and spectrophotometric analysis of third generation lightemitting diod (LED) of light curing unit. J Contemp Dent Prac 2007:8;43-51.
- Price RB, Drand T, Sedarous M, Andreou P, Loney RW. Effect of distance on the power density from two light guides. J Esthet Dent 2000;12:320-327.
- Knobloch L, Kerby RE, Clelland N, Lee J. Hardness and degree of conversion of posterior packable composites. Oper Dent 2004;29:642-649.
- Mills RW, Uhl A, Black well GB. High power light emmiting diod (LED) arrays versus halogen light polymerization of oral bio materials: Bascol hardness, compressive strength and radiometric properties. Biomat 2002; 23: 2955-2963
- Uhl A, Mills RW, andt KD. Polymerization and light induced heat of dental composite cured with LED and halogene technology. Biomet 2003;24:1809-1820.
- Shortall AC, Harrington E, Wilson HJ. Light curing unit effectiveness assessed by dental radiometers. J Dent 1995; 23:227-232.
- Al Mazrok MI. The effect of wrapping of light-cure tips on the cure of composite resin. Eur J Gen Dent 2012; 1:83-86.
- Leonard DL, Charlton DG, Hilton TJ. Effect of curingtip diameter on the accuracy of dental radiometers. Oper Dent 1999; 24:31-37.
- Chong SL, Lam YK, Lee FK, Ramalingam L, Yeo AC, Lim CC. Effect of various infection-control methods for light-cure units on the cure of composite resins. Oper Dent 1998;23:150-154
- McAndrew R, Lynch CD, Pavli M, Bannon A, Milward P. The effect of disposable infection control barriers and physical damage on the power output of light curing units and light curing tips. Br Dent J 2011;210:E12.