
Plaque Score During Orthodontic Treatment In Relation To Age And Gender
INTRODUCTION
It is important to maintain better oral hygiene during orthodontic treatment. Fixed orthodontic appliances cause difficulty in tooth brushing which lead to accumulation of plaque. Emphasis must be given on oral hygiene maintenance, including both professional tooth cleaning and home care instructions1-3.
There is direct correlation between oral hygiene and periodontal health4. Orthodontic appliances such as brackets and bands trap food and other debris under wire which makes it challenging for patient to maintain oral hygiene5. Good oral hygiene is hallmark for good dental and periodontal health during orthodontic treatment6-8. Brackets, arch wires and other orthodontic gadgets are main focal points for accumulation of plaque and also acts as obstacle to control the plaque hence enhancing gingivitis9. Plaque also carries cariogenic bacteria which are capable of developing white spot lesions around brackets margins7,8. Fixed orthodontic treatment increases risk of enamel demineralization which is evident in patients with compromised oral hygiene10.
A recent review of literature concluded that fixed orthodontic treatment may cause few detrimental effects to the periodontium11. Along with that in another study it is also stated that periodontitis due to orthodontic fixed appliance therapy may be avoided if basic oral hygiene maintenance protocol is followed12. It is observed that a significant percentage of orthodontic patients feel difficulty in maintaining oral hygiene and exhibit adverse effects13.
Tooth brushing is the principal tool used for plaque control, however regular toothbrush does not remove inter-dental plaque adequetly14.Therefore inter-dental plaque controlling aids such as flossing and inter-dental brushing should be added along with regular brush. Oral hygiene instructions are frequently demonstrated by orthodontists to their patients routinely to motivate them for oral hygiene improvement15. Aim of our research was to assess the plaque score in the fixed orthodontic patients in relation to gender, age and duration of orthodontic treatment.
METHODOLOGY
A cross sectional study was conducted from spetember 2013 to march 2014 at the Department of Orthodontics, Liaquat Medical University Hospital and private orthodontic clinics in Hyderabad. Permission was obtained from the ethical review committee and informed written consent was taken from all participants.
The online Epi calculator was used to calculate sample size. The sample size was calculated at a 95% confidence interval, with 0.3% estimated proportion of plaque and 0.05 desired precision of estimate from the 1000 population size. The required sample size was 245.
Non-probability purposive sampling technique was used to select 245 orthodontic patients. Orthodontics patients having fixed orthodontics appliances, age ranges from 13 to 25 years of either gender, permanent dentition up to 2nd molar, having no enamel defects or no restorations involving facial surface and good general health were included in study. Patients having crown, bridge, removable appliances or clear liners and mouth washes used in last four weeks were excluded from study.
Mouth mirror and profound light were used to examine patients individually. Selected patients were asked to chew the plaque disclosing tablet (Eviplac Pastilhas), swish it for thirty seconds, spit out and wash once with clean water to decrease the false positive results. Facial, palatal and lingual surfaces were examined to calculate the plaque score. Turseky modification of Quigley Hein Plaque index was used to calculate plaque score using the following formulae:
Index = Total score / number of surfaces Examined The data was analyzed by Statistical Package for Social Sciences (SPSS) version 16. Categorical variables like gender and cleaning of teeth are presented in frequencies. Numerical variables like age and plaque score were recorded as mean and SD. Independent T test was used to check significance of plaque score in male and female. One way ANOVA test was applied among plaque score and duration of fixed appliance to assess the plaque score. Correlation analysis was done between the age of patients and plaque index score. The level of significance was set to < 0.05 at 95% Confidence Interval.
RESULTS
Mean plaque score was 4.29+1.58 and mean age 19.1+2.47 years. Mean values of plaque for male 2.42+0.70 and female 2.51+1.99 were statistically not significant. (Table-1).
Male and female patients were 42% and 58% respectively. Majority of Male and female patients were cleaning their teeth once a day and very less number of patients were cleaning their teeth thrice a day. (Table-2)
The analysis of variance (ANOVA) test showed insignificant differences in plaque score and duration of fixed appliance. (Table-3)
There was insignificant (r=0.035, p = 0.581) correlation between age and plaque score. (Table-4)
 Table-1: Plaque Score in Male and Female
Table-1: Plaque Score in Male and Female
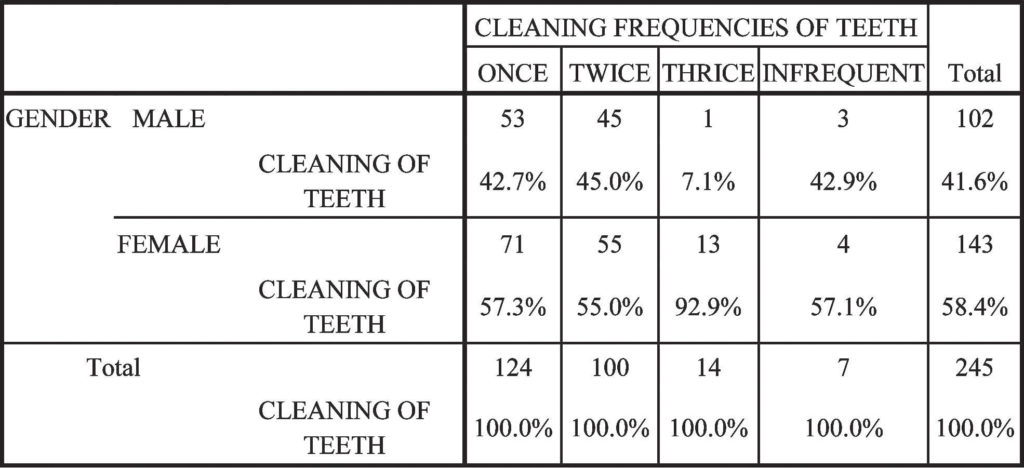 Table-2: Cross Tabulation Between Gender and Cleaning Frequencies of Teeth
Table-2: Cross Tabulation Between Gender and Cleaning Frequencies of Teeth
 Table-3: Plaque Score and Duration of Fixed Appliance.
Table-3: Plaque Score and Duration of Fixed Appliance.
 Table-4: Correlation Between Age and Plaque Score
Table-4: Correlation Between Age and Plaque Score
DISCUSSION
For the correction of skeletal, dental and facial problems an effective cooperation is required between orthodontist, hygienist, patient and specialist of related fields linked to that problem16. If patient is motivated and keen to control plaque effectively he may keep his dentition for life time17. Orthodontic treatment becomes complicated and develop undesirable effects if oral hygiene is not maintained18.
Most of the periodontal diseases and dental caries are caused by plaque. Therefore, plaque control must be insisted in avoiding periodontal problems during orthodontic treatment4.
There was insignificant difference of plaque score between different genders. The findings of this study are in agreement with the study of Sukhia HR19 and Attasi F, Awartani F20. In comparison of brushing frequency, females brushed more than male counterparts which can be compared with the research of Sukhia HR19 and Da’ameh M D21. This might be due to the fact that females are more conscious about their hygiene as compared to males. Very few patients were irregular in cleaning their teeth on daily basis.
The current study found that plaque score does not increase with increase in treatment duration, this finding is not in harmony with other studies9-22,24. Optimal oral hygiene can be achieved when proper measures are used25-26.
There was insignificant (r=0.035, p = 0.581) correlation between age and plaque score. This finding was in contrast with the study results of Al-Hadad KA et27 al and a study conducted on subjects in Sana’a28. However some
researchers have reported similar results as ours 29,30. These variations may be attributed to differences in methodology or age of study samples and may also reflect genuine differences in oral hygiene practices, culture, and food habits. This study was conducted on orthodontic fixed appliances patients so the results of our research may not be valid for patients using clear aligners and removable appliances. The data was collected by single researcher so operator bias could not be eliminated.
CONCLUSION
It is concluded that:
- Plaque score was not influenced by age or gender of our study subjects
- Plaque score did not increase with increased duration of orthodontic treatment.
REFRENCES
- Gold SL. Plaque-control motivation in orthodontic practice. Am J Orthod. 1975 ;68:8-14.
- Clark JR. Oral hygiene in the orthodontic practice: Motivation, responsibilities, and concepts. Am J Orthod. 1976 ;69:72-82.
- Yeung SC, Howell S, Fahey P. Oral hygiene program for orthodontic patients. Am J Orthod Dentofacial Orthop. 1989 ;96:208-213.
- Kloehn JS, Pfeifer JS. The effect of orthodontic treatment on the periodontium. Angle Orthod 1974;44:127134.
- RafeZvi, Vardimon Alexander, Ashkenazi Malka. Comparative study of 3 types of toothbrushes in patients with fixed orthodontic appliances. Am J Orthod Dentofac Orthop 2006;130: 92-95.
- Zachrisson BU. Cause and prevention of injuries to teeth and supporting structures during orthodontic treatment. Am J Orthod 1976;69: 285-300.
- Mitchell L. Decalcification during orthodontic treatment with fixed appliances: An overview. Br J Orthod 1992;19:199-205.
- Atack NE, Sandy JR, Addy M. Periodontal and microbiological changes associated with the placement of orthodontic appliances: A review. J Periodontol 1996;67:78-85.
- Zachrisson S, Zachrisson BU. Gingival condition associated with orthodontic treatment. Angle Orthod 1972;42:26-34.
- Costa MR, da Silva VC, Miqui MN, Colombo AP, Cirelli JA. Effects of ultrasonic, electric, and manual toothbrushes on subgingival plaque composition in orthodontically banded molars. Am J Orthod Dentofacial Orthop. 2010;137:229-235
- Boyd R. enhancing the value of orthodontic treatment: incorporating effective preventive dentistry into treatment. Am J Orthod 2000:117;601-603.
- Laher A, Kroon J, Booyens SJ. Effectiveness of four manual toothbrushes in a cohort of patients undergoing fixed orthodontic treatment in an academic training hospital. SADJ. 2003;58:231, 234-237.
- Quigley GA, Hein JW. Comparative cleansing efficiency of manual and power brushing. J Am Dent Assoc. 1962;65:26-29.
- Bimstein E, Needleman HL, Karimbux N, Van Dyke TE. Periodontal and gingival health and diseases. London NW1 0AE: Martin Dunitz Ltd; 2001
- Lees A, Rock WP. A comparison between written, verbal, and videotape oral hygiene instruction for patient with fixed appliances. J Orthod 2000;27:323-328.
- Kharsa MAI. The importance of oral hygiene in orthodontic treatment. The Orthodontic SYPER J, 2007.
- Schwaninger B, Vickers-Schwaninger N. Developing an effective oral hygiene program for the orthodontic patient: review, rationale, and recommendations. AM J Orthod1979;75:447-452.
- Machen, DE. Periodontal evaluation and updates: don’t abdicate your duty to diagnose and supervise. Am J Orthod DentofacOrthoped 1990;98:84-85.
- Sukhia HR. Oral hygiene evaluation in orthodontic practice. Pak Oral Dent J. 2002;22:31-38.
- Attasi F, Awartani F. Oral hygine status among orthodontic patients. J Contemp Dent Pract 2010;11:2532.
- Da’ameh M D, Al-Shorman I, Al-Shdeifat N, Fnaish MM. Oral hygiene measures in orthodontic treatment in Northern Jordan. Pak Ora Dent J.2011;31:336-339.
- Zachrisson BU. Clinical implications of recent orthodontic periodontic research findings. Semin Orthod 1996;2:4-12.
- Huser MC, Baehni PC, Lang R. Effects of orthodontic bands on microbiologic and clinical parameters. Am J Orthod Dento facial Orthop 1990;97:213-218.
- Kloehn JS, Pfeifer JS. The effect of orthodontic treatment on the periodontium. Angle Orthod 1974;44:127134.
- Speer C, Pelz K, Hopfenmuller W, Holtgrave EA. Investigations on the influencing of the subgingivalmicroflora in chronic periodontitis. A study in adult patients during fixed appliance therapy [in English and German]. J Oro fac Orthop 2004;65:34-47.
- McGlynn FD, LeCompte EJ, Thomas RG, Courts FJ, Melamed BG. Effects of behavioral self-management on oral hygiene adherence among orthodontic patients. Am J Orthod Dento facial Orthop 1987;91:15-21.
- Al-Haddad KA, Ibrahim YT, Al-Haddad AM, AlHebshi NN. Assessment of Gingival Health Status among 5- and 12-Year-Old Children in Yemen: A Cross-Sectional Study. ISRN dentistry 2013 (2013).
- Clerehugh, U. Laryea, and H. V. Worthington, “Periodontal condition and comparison of toothcleaning using chewing sponge, chewing sticks and toothbrushes in 14-year-old schoolchildren in Ghana, Commun Dent Oral Epidemiol 1995 23:319-320.
- Cahen PM, Turlot JC, Frank RM, Obry-Musset AM. National survey of caries prevalence in 6-15-year-old children in France. J Dent Res. 1989;68:64-68.
- R. D. Emslie, A dental health survey in the Republic of the Sudan, Brit Dent J, 1966; 120:167-178.